
Abstract
Objectives
The objective of this study was to assess the influence of an iterative CT reconstruction algorithm (IA), newly available for CT-fluoroscopy (CTF), on image noise, readers’ confidence and effective dose compared to filtered back projection (FBP).
Methods
Data from 165 patients (FBP/IA = 82/74) with CTF in the thorax, abdomen and pelvis were included. Noise was analysed in a large-diameter vessel. The impact of reconstruction and variables (e.g. X-ray tube current I) influencing noise and effective dose were analysed by ANOVA and a pairwise t-test with Bonferroni–Holm correction. Noise and readers’ confidence were evaluated by three readers.
Results
Noise was significantly influenced by reconstruction, I, body region and circumference (all p ≤ 0.0002). IA reduced the noise significantly compared to FBP (p = 0.02). The effect varied for body regions and circumferences (p ≤ 0.001). The effective dose was influenced by the reconstruction, body region, interventional procedure and I (all p ≤ 0.02). The inter-rater reliability for noise and readers’ confidence was good (W ≥ 0.75, p < 0.0001). Noise and readers’ confidence were significantly better in AIDR-3D compared to FBP (p ≤ 0.03). Generally, IA yielded a significant reduction of the median effective dose.
Conclusion
The CTF reconstruction by IA showed a significant reduction in noise and effective dose while readers’ confidence increased.
Key Points
• CTF is performed for image guidance in interventional radiology.
• Patient exposure was estimated from DLP documented by the CT.
• Iterative CT reconstruction is appropriate to reduce image noise in CTF.
• Using iterative CT reconstruction, the effective dose was significantly reduced in abdominal interventions.
Similar content being viewed by others
Introduction
During the last decade, minimally invasive procedures performed by means of computed tomography fluoroscopy (CTF) image guidance became state-of-the-art procedures for different diagnostic and therapeutic interventions [1–5]. Despite all the advantages of real-time image guidance during the intervention, CTF is associated with radiation exposure to the patient and subsequent exposure to the interventional radiologist (IR) by scattered photons [6–8]. Particularly in complex CTF-guided interventions (e.g. radiofrequency ablation [RFA]), high patient skin doses up to 1–2 Gy were reported [9, 10], reaching the threshold dose for deterministic effects [8, 10, 11].
In parallel, the risk of a radiation-induced cancer disease associated with CT exposure is well known from diagnostic applications [12, 13]. This risk has to be discussed seriously regarding CTF used in image-guided diagnostic procedures, such as biopsies or therapies (e.g. RFA or microwave ablation [MWA]), which are frequently performed with a potentially curative intent.
One immanent problem in the dose-oriented optimisation of CTF-guided interventions is the drastically increased image noise for decreasing X-ray tube current in low-dose CT [14, 15]. Until recently, new reconstruction technologies (e.g. iterative CT reconstructions) were only available for diagnostic CT imaging [16–18] and for low-dose-applications (e.g. contrast-enhanced CT angiography) [19, 20]. Depending on the diagnostic CT application, iterative reconstruction algorithms demonstrated the opportunity for dose reduction of 30–75% with preserved image quality [21, 22]. In contrast, image reconstruction in CTF is always performed by FBP.
This study’s purpose was to compare a newly available iterative image reconstruction algorithm (AIDR 3D) with the current standard FBP regarding the image quality of the CTF and the resulting effective dose to the patients.
Material and methods
Patients
Data of 206 interventional procedures performed between March and June 2015 at our department were screened for analysis. The data of 50 interventions had to be excluded from the analysis (e.g. because of metal artefacts in the reference region, e.g. thoracic or abdominal aorta, n = 45; the reference region not imaged by CTF, n = 4; 4-year-old child, n = 1). Altogether, the data of 125 adult patients (M/F: 76/49; mean age: 65.4 ± 11.5 years, range: 32.8–88.1) with a total of 156 CTF-guided procedures were included in the analysis (Table 1).
Image reconstruction of the CTF was performed by FBP in 72 patients and, after an upgrade of the CT system software to AIDR 3D, in 65 patients, respectively. 104 underwent a single intervention, 17 patients underwent two interventions and three patients underwent three timely independent CTF-guided interventions in the study period. A single patient underwent four consecutive CTF-guided interventions. No patient had more than one CTF-guided intervention in the same body region, which was reconstructed with the same algorithm (FBP or AIDR 3D). The circumference of the body region imaged by CTF was measured in all patients. Additionally, the body mass index (BMI) was taken from the clinical documentation for each patient. In case only part of the patient´s cross-section was visualised by CTF, the circumference was measured in a previously acquired diagnostic CT image corresponding to the CTF slice.
The study was approved by the local ethics committee (registration number: 18/16), and the patients provided written informed consent on the anonymised evaluation of their image and dose exposure data. All CTF-guided interventions were part of the routine clinical workflow.
CT fluoroscopy
Imaging was performed with an 80-row CT (Aquilion PRIME, Toshiba Medical Systems Corporation, Otawara, Japan). CTF was performed with an X-ray tube voltage of 120 kVp and a rotation speed of 0.5 s, a reconstructed image matrix of 512 x 512 and a slice thickness of 6 mm. The X-ray tube current (I) was individually chosen for each patient taking into account the prerequisite of the IR balancing between the image quality necessary for CTF-based navigation (e.g. defined by image noise, detectability of organ contours and target structures, and depiction of puncture needles) and CT exposure. Imaging was performed without dose modulation or an automatic exposure control system. The CTF procedures were performed by a total of 14 IRs, with a median of five interventions per IR (interquartile range [IQR] = 1/18, range: 1–37), who had at least 6 months of experience with CTF. The CTF of the first cohort (n = 72 patients) was reconstructed with FBP. After a system upgrade (System Software, version 6.0, Toshiba Medical Systems Corporation), the CTF images were reconstructed with AIDR 3D, an iterative image reconstruction algorithm newly available for CTF in a second cohort (n = 65 patients). Other system parameters were not affected by the upgrade.
Region-of-interest analysis
The impact of the reconstruction algorithms (FBP and AIDR 3D) and the selected X-ray tube current on the image noise of the CTF scans was quantified by a region-of-interest (ROI) analysis. The ROI was placed in a large-diameter vessel (e.g. the aorta) in the thoracic-abdominal region or the common iliac or femoral artery in the pelvis. Blood within the vessel is inherently texture free and features homogeneous tissue attenuation (Hounsfield units [HU]) in native CTF scanning [23]. Thus, any deviation in HU represents image noise. The diameter of a circular ROI was set manually within the centre of the vessel to prevent integration of HU values of the surrounding tissue or artificial information (e.g. from vessel calcifications). Its diameter was chosen to cover about 75% of the diameter of the vessel (see Supplementary Data, Table 1). Image noise was quantified by determining the standard deviation of HU values inside the ROI [23, 24]. ROI analysis was performed by ImageJ V1.5b [25].
Blinded reading
Three readers (minimum of 7 years of experience in CTF) blinded to the reconstruction algorithms independently scored CTF scans for image noise and readers’ confidence using the presented CTF image quality for navigation. Each parameter was rated with a 5-point Likert scale (Table 2). Reading was performed using Osirix MD V7.0 [26].
Effective dose from CTF
The impact of the reconstruction algorithms on the patients’ radiation exposure from CTF was evaluated by deriving the effective dose from the DLP [27]. DLP values, based on a cylinder phantom of polymethylmethacrylate (PMMA) with a diameter of 320 mm (body geometry), were documented for each interventional procedure by the CT device. The effective CT exposure (E eff) was calculated by weighting the DLPtotal from the CTF procedure with a body region specific conversion factor κ [28]:
The body region specific conversion factor (κ Region) was chosen in accordance with Bongartz et al. [29] and Shrimpton et al. [30] (κThorax = 0.014 mSv/(mGy*cm), κAbdome and κPelvis = 0.015 mSv/(mGy*cm)).
Statistics
The R software package (version 3.1.3; R Foundation for Statistical Computing, Vienna, Austria) was used for statistical analysis. Descriptive parameters were expressed as mean ± standard deviation, median, interquartile range (IQR) and range. The applied X-ray tube current was subdivided into two groups (factor levels: I ≤45 mA, and I >45 mA) to test its impact on image noise. Likewise, the circumferences of the patients were subdivided into two groups (factor levels: ≤100 cm and >100 cm) to estimate the effect of body circumference on image noise [31]. ANOVA was employed to assess the impact of the factors reconstruction algorithm, body region, patient circumference and X-ray tube current on the image noise and on the effective dose cumulated from CTF. Furthermore, the impact of the fluoroscopic procedure (e.g. interstitial brachytherapy, drainage placement or biopsy) on the effective dose was included into ANOVA. The effects from factor levels on the image noise and on the effective dose were tested by employing the paired t-test with Bonferroni–Holm correction for multiple comparisons.
The inter-rater agreement on image noise scores and readers’ confidence scores were calculated by Kendall's Coefficient of concordance (W). Differences in the scores for FBP and AIDR 3D were tested for significance by the unpaired Mann-Whitney test (two sample Wilcoxon test).
A p-value of 0.05 (two-tailed) was set as the level of statistical significance.
Results
Patient cohort
There was no significant difference with regards to age, body mass index (BMI) and body circumference between the patient cohorts with FBP and AIDR 3D CTF images (p ≥ 0.54) (Table 1). CTF-guided interventions included the placement of drainage tubes (n = 53), biopsies (n = 78), MWA or RFA (MWA + RFA: n = 6) and interstitial placement of brachytherapy catheters (n = 19) (Table 3).
Image noise
Image noise was determined in the thoracic, abdominal and pelvic interventions in n = 28 (FBP/AIDR 3D: 12/16), n = 108 (FBP/AIDR 3D: 61/47) and n = 20 (FBP/AIDR 3D: 9/11) cases, respectively (Table 3). ANOVA showed a significant interdependency between image noise and the reconstruction algorithm (p = 0.0002), X-ray tube current (p = 0.0001), imaged body region (p < 0.001) and circumference of the imaged body region (p < 0.001) (Table 4). Across all the data, the image noise was significantly lower in the CTF images reconstructed by AIDR 3D compared to FBP reconstruction (p = 0.02). Significant interactions of these parameters were observed (Table 4), which are presented by interaction plots (Fig. 1a–d).

Interaction plots between (a) algorithm and image noise in patients with a smaller body circumference and (b) larger body circumference, and interaction plots between (c) reconstruction algorithm and X-ray tube current for smaller body circumference and (d) larger body circumference. AIDR 3D adaptive iterative dose reduction 3D, FBP filtered back projection. Note: values are given as mean ± SD, number of cases is given in parenthesis
The effect from the body region on image noise in CTF did not differ significantly in the abdominal and pelvic regions (p = 1.0), whereas image noise was significantly lower in CTF of thoracic interventions compared to abdominal and pelvic interventions (all p < 0.0001). The effect from the reconstruction algorithm on the image noise in CTF was not significant in patients with a small body circumference (thorax: p = 0.41, abdomen: p = 0.12, pelvis: p = 0.09, Fig. 1a). In contrast, for patients with a larger body circumference (>100 cm, Fig. 1b), AIDR 3D reconstruction yielded a significant reduction of the image noise level for CTF-guided interventions in all body regions (mean reduction; abdomen: 23.7% [p = 0.03], pelvis: 29.1% [p = 0.01], thorax: 40% [p = 0.04]).
Image quality in CTF reconstructed by means of FBP and AIDR 3D is exemplified for different body regions in patients with comparable body circumferences (Fig. 2a–f).

CT fluoroscopy (CTF) with filtered back projection (FBP) (left) and Adaptive Iterative Dose Reduction 3D (AIDR 3D) (right). Body regions were demonstrated in patients with comparable circumferences. Thoracic region: (a) in a patient (F, 73.7 years old, body circumference = 104 cm, I = 30 mA) for biopsy of a pulmonary lesion and (b) a patient (M, 70.4 years old, body circumference = 108 cm, I = 30 mA) for drainage placement. Abdominal region: (c) in a patient (F, 50.9 years old, body circumference = 84 cm, I = 60 mA) for biopsy of a lymph node and (d) a patient (F, 56.1 years old, body circumference = 88 cm, I = 30 mA) for biopsy of a liver lesion. Pelvic region: (e) in a patient (M, 69.3 years old, body circumference = 98 cm, I = 60 mA) for biopsy of a lymph node and (f) a patient (M, 72.0 years old, body circumference = 94 cm, I = 30 mA) for drainage placement
Results from the blinded reading showed a good inter-rater reliability for image noise (W = 0.75, p < 0.0001) and readers’ confidence (W = 0.78, p < 0.0001). With regard to image noise (reduction), CTF reconstructed by AIDR 3D was rated significantly better than CTF reconstructed by FBP (mean difference = 0.30, p = 0.0004, Table 5). Readers’ confidence was also scored higher in AIDR-3D reconstructions (mean difference = 0.19, p = 0.03, Table 5).
Effective dose
For the evaluation of the effective dose, the data of nine technical exceptional demanding interventional procedures (n = 1 thoracic and n = 4 abdominal biopsies, and n = 4 abdominal and pelvic drainage placements) were excluded from the analysis to prevent a bias resulting from a prolonged intervention time deviating significantly from the standard procedure. These procedures were characterised by incompliance of the patient (n = 2) or were a combination of diagnostic/therapeutic interventional procedures (e.g. biopsy in several regions and subsequent and drainage placement, n = 7).
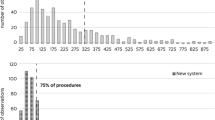
ANOVA showed a significant interdependency between the effective dose (Table 6) and the reconstruction algorithm (p = 0.0002), imaged body region (p = 0.02), type of intervention (p < 0.0001) and X-ray tube current (p = 0.001). The corresponding X-ray tube current values used for CTF in the different body regions and the significance of differences are specified in Table 7. Furthermore, significant interactions of these parameters were observed (Table 6). The effect of the different parameters on the effective dose is illustrated by interaction plots (Fig. 3a, b).

Interaction plots between (a) body region and effective dose accumulated by CT fluoroscopy (CTF) and (b) interventional procedure and effective dose from CTF for both reconstruction algorithms (all data). Additionally, the interaction between (c) the interventional procedure and effective dose is shown for the abdominal region, solely. AIDR 3D Adaptive Iterative Dose Reduction 3D, FBP filtered back projection, MW microwave ablation, RFA radiofrequency ablation, Biop biopsy
The highest effective doses were observed for the placement of brachytherapy catheters in solid tumours of the liver (p = 0.02) (Fig. 3b). MWA or RFA resulted in a higher dose exposure to the patient than drainage placements and diagnostic biopsies (p < 0.03) (Fig. 3b). The effective dose did not differ significantly between drainage placement and biopsy (p = 1.0) (Fig. 3b). Across all of the procedures and body regions, the effective dose of CTF was significantly lower in the interventions employing the AIDR 3D reconstruction algorithm compared to the interventions employing FBP reconstruction (p = 0.005). The extent of dose reduction varied for the body region and the interventional procedure (Figs. 3a, b). This finding is illustrated for CTF-guided interventions in the abdomen, where the highest reduction of dose exposure could be found (Fig. 3c).
Implementation of the AIDR 3D algorithm yielded a reduction of the median effective dose imposed on the patient by CTF of approximately 50% for abdominal biopsies (FBP = 11.0 mSv, AIDR 3D = 5.5 mSv, p = 0.01) (Fig. 4a) and of 60% for the interstitial placement of brachytherapy catheters in the liver (FBP = 49.7 mSv, AIDR 3D = 19.2 mSv, p = 0.04) (Fig. 4b). No reduction of the median effective dose of CTF by the AIDR 3D algorithm could be detected for thoracic biopsies (FBP = 5.1 mSv, AIDR 3D = 5.2 mSv, p = 0.96) (see Supplementary Data). For the placement of drainage catheters in the abdomen and pelvis, the implementation of AIDR 3D showed a trend toward reduction of the median effective dose (abdomen: FBP = 4.7 mSv, AIDR 3D = 3.6 mSv, p = 0.4; pelvis: FBP = 6.1 mSv, AIDR 3D = 4.6 mSv, p = 0.62) (see Supplementary Data). The effect from FBP and AIDR 3D on the effective dose was not evaluated for MWA and RFA (FBP: n = 3, AIDR 3D: n = 2) and the remaining combinations of interventional procedures and body regions due to the limited number of cases.

Effective dose from CT fluoroscopy (CTF)-guided procedures in the abdomen for: (a) biopsies and (b) the placement of brachytherapy catheters. AIDR 3D Adaptive Iterative Dose Reduction 3D, FBP filtered back projection
Discussion
We examined the influence of an iterative 3D image reconstruction algorithm, newly available for CTF, on image quality and effective dose exposure accumulated by the patients in clinical applications, such as biopsies, drainage tube placements or interstitial tumour ablations. Furthermore, independent blinded readers evaluated image noise and readers’ confidence.
Compared to the standard FBP algorithm, the newly available AIDR 3D algorithm yielded a reduction in X-ray tube current while preserving or even reducing image noise, especially in patients with a large body circumference in the imaged region. In accordance with the reduction of the X-ray tube current, a reduction of effective patient dose exposure from CTF could be demonstrated. The extent of the reduction of the effective dose exposure varied for different CTF procedures. To the best of our knowledge, this is the first study to show these effects.
A significant effect from the patient size (circumference) was detected in image noise analysis and X-ray tube current. For patients with a small body circumference (≤100 cm), AIDR 3D reconstruction yielded a similar image noise level compared to FBP in CTF-guided interventions in the abdomen and pelvis, employing just a fraction of the X-ray tube current. In contrast, AIDR 3D reconstruction yielded no significant effect in image noise levels and X-ray tube current in CTF-guided interventions in the thorax for these patients. This effect can be attributed to the lower attenuation and the a priori low X-ray tube current used in FBP-based CTF in the thoracic region.
In total, image noise and readers’ confidence were not only preserved by using AIDR 3D. Moreover, observers independently scored a reduction in image noise and an increase in diagnostic confidence. This has to be addressed for further optimisation of dose exposure.
Generally, an increase in image noise can be expected in CTF when the X-ray tube current is decreased. A dependency of ~ 1/√I was observed from diagnostic CT imaging [24] and low-dose-CT applications [14] for FBP and iterative algorithms. The significant reduction of image noise and the corresponding potential for X-ray tube current reduction is a typical property of an iterative reconstruction algorithm [14, 22, 32, 33].
In addition to the improvement in image noise, we observed a significant reduction of the effective dose from CTF. In contrast to the image noise, which reflects the immediate impact of the reconstruction algorithm on image quality, the effective dose applied to the patient also includes the complexity of the interventional procedure (e.g. MWA/RFA vs. biopsy) and the corresponding CTF time. We showed a significant reduction of the effective dose in the abdominal region for a variety of interventional procedures by using AIDR 3D while the effective dose accumulated by the patients from CTF using FBP (Supplementary Data) compared well to other published reports (e.g. Kloeckner et al.) [6].
The optimised dose management for patients also addresses the IR dose exposure from scattered photons. Although standard radiation protection equipment (e.g. lead drapes on top of the patient to reduce scatter [8, 34], needle holders [2, 35–38] and body and lens shielding of the IR [39]), as well as technical innovations (e.g. sectorial modulation of the X-ray tube current to reduce the direct back scattering of photons from the patient to the IR [40]) were routinely implemented, further optimisations were often limited due to the technical aspects of the CT scanner. Different authors assessed the significant dimension of professional dose exposure from CTF [2, 3, 8]. Nawfel et al. [8] observed for a specific CTF protocol (120 kVp, 50 mA, 10 mm collimation) scattered exposure rates of 27 and 1.2 μGy/sec at 10-cm and 1-m distances to the scanning plane. Kim et al. [3] measured the effective dose exposure of the IR with thermoluminescent dosimeters in biopsies of pulmonary lesions. The authors found a whole body exposure of 0.054 mSv and a hand-dose exposure of the IR of 0.759 mSv per intervention, respectively. The observed dose exposures estimated by phantom measurements or from clinical applications illustrate the importance of a further dose reduction for radiation safety aspects. It can be hypothesised that the level of dose reduction observed for AIDR 3D will reflect the dose reduction for the IRs by using the specific iterative image reconstruction.
A limitation of our study is the model-based estimation of the patient exposure. Our analysis used the DLP, documented by the CT scanner dose report, to estimate the corresponding effective dose by an established procedure reported by the International Commission on Radiological Protection (ICRP) Publication No. 102 [39]. This approach was chosen to reduce the complexity in comparing different scan protocols (e.g. X-ray tube current settings and total scan time) to an estimation of exposure values for the CTF procedure and did not reflect the individual patient's habits.
A further limitation is the limited number of cases and different combinations of interventional procedures in various body regions. Thus, the quantity of observations was not sufficient for statistical analysis of the impact of either reconstruction algorithm in every body region. Finally, it is necessary to reflect on the influence from ROI size, defined by the different sizes of the reference regions, on image noise estimated from standard deviation as a surrogate parameter. From our data, we observed an ROI area approximately two times smaller in the pelvis compared to those of the thorax and abdomen (Supplementary Data, Table 1), resulting in an overestimation of the noise level in the pelvis by a factor of √2. This limitation is inherent due to the employed methodology and must be taken into account for the comparison of results between body regions. For intra-region assessment, the effect was not significant (p > 0.11).
In conclusion, the advantage of AIDR 3D in CTF compared to FBP reconstruction is the reduction of image noise and the increase in readers’ confidence. The application of AIDR 3D also provides an opportunity to reduce CT radiation exposure from fluoroscopic procedures without a significant impairment of image quality. The corresponding decrease in X-ray tube current resulted in a significant reduction of the dose exposure of the patient. Further studies are necessary to assess the impact of dose reduction to the staff’s exposures.
Abbreviations
- AIDR 3D:
-
Adaptive Iterative Dose Reduction 3D
- ANOVA:
-
Analysis of variance
- BMI:
-
Body mass index
- CTF:
-
CT fluoroscopy
- DLP:
-
Dose length product
- FBP:
-
Filtered back projection
- HU:
-
Hounsfield units
- I:
-
X-ray tube current
- IQR:
-
Interquartile range
- IR:
-
Interventional radiologist
- MWA:
-
Microwave ablation
- PMMA:
-
Polymethylmethacrylate
- RFA:
-
Radiofrequency ablation
- ROI:
-
Region of interest
References
Froelich JJ, Ishaque N, Regn J, Saar B, Walthers EM, Klose KJ (2002) Guidance of percutaneous pulmonary biopsies with real-time CT fluoroscopy. Eur J Radiol 42:74–79
Silverman SG, Tuncali K, Adams DF, Hooton S, Tuncali K, Adams DF (1999) CT fluoroscopy-guided abdominal interventions: techniques, results, and radiation exposure. Radiology 212:673–681
Kim GR, Hur J, Lee SM et al (2011) CT fluoroscopy-guided lung biopsy versus conventional CT-guided lung biopsy: a prospective controlled study to assess radiation doses and diagnostic performance. Eur Radiol 21:232–239
Carlson SK, Bender CE, Classic KL et al (2001) Benefits and safety of CT fluoroscopy in interventional radiologic procedures. Radiology 219:515–520
Prosch H, Stadler A, Schilling M et al (2012) CT fluoroscopy-guided vs. multislice CT biopsy mode-guided lung biopsies: accuracy, complications and radiation dose. Eur J Radiol 81:1029–1033
Kloeckner R, dos Santos DP, Schneider J, Kara L, Dueber C, Pitton MB (2013) Radiation exposure in CT-guided interventions. Eur J Radiol 82:2253–2257
Pereira MF, Alves JG, Sarmento S et al (2011) Preliminary assessment of the dose to the interventional radiologist in fluoro-CT-guided procedures. Radiat Prot Dosim 144:448–452
Nawfel RD, Judy PF, Silverman SG et al (2000) Patient and personnel exposure during CT fluoroscopy-guided interventional procedures. Radiology 216:180–184
Tsalafoutas IA, Tsapaki V, Triantopoulou C, Gorantonaki A, Papailiou J (2007) CT-guided interventional procedures without CT fluoroscopy assistance: patient effective dose and absorbed dose considerations. Am J Roentgenol 188:1479–1484
Joemai RMS, Zweers D, Obermann WR, Geleijns J (2009) Assessment of patient and occupational dose in established and new applications of MDCT fluoroscopy. Am J Roentgenol 192:881–886
Wagner LK, Eifel PJ, Geise RA (1994) Potential biological effects following high X-ray dose interventional procedures. J Vasc Interv Radiol 5:71–84
Berrington de González A, Darby S (2004) Risk of cancer from diagnostic X-rays: estimates for the UK and 14 other countries. Lancet 363:345–351
National Council on Radiation Protection (2009) Ionizing radiation exposure of the population of the United States. National Council on Radiation Protection and Measurements, Bethesda, MD
Grosser OS, Kupitz D, Ruf J et al (2015) Optimization of SPECT-CT Hybrid Imaging Using Iterative Image Reconstruction for Low-Dose CT: A Phantom Study. PLoS ONE 10, e0138658
Xia T, Alessio AM, De Man B, Manjeshwar R, Asma E, Kinahan PE (2012) Ultra-low dose CT attenuation correction for PET/CT. Phys Med Biol 57:309–328
Martinsen ACT, Sæther HK, Hol PK, Olsen DR, Skaane P (2012) Iterative reconstruction reduces abdominal CT dose. Eur J Radiol 81:1483–1487
Sagara Y, Hara AK, Pavlicek W, Silva AC, Paden RG, Wu Q (2010) Abdominal CT: comparison of low-dose CT with adaptive statistical iterative reconstruction and routine-dose CT with filtered back projection in 53 patients. Am J Roentgenol 195:713–719
Hara AK, Paden RG, Silva AC, Kujak JL, Lawder HJ, Pavlicek W (2009) Iterative reconstruction technique for reducing body radiation dose at CT: feasibility study. Am J Roentgenol 193:764–771
Leipsic J, Labounty TM, Heilbron B et al (2010) Estimated radiation dose reduction using adaptive statistical iterative reconstruction in coronary CT angiography: the ERASIR study. Am J Roentgenol 195:655–660
Gebhard C, Fuchs TA, Fiechter M et al (2013) Image quality of low-dose CCTA in obese patients: impact of high-definition computed tomography and adaptive statistical iterative reconstruction. Int J Cardiovasc Imaging 29:1565–1574
Singh S, Kalra MK, Do S et al (2012) Comparison of hybrid and pure iterative reconstruction techniques with conventional filtered back projection: dose reduction potential in the abdomen. J Comput Assist Tomogr 36:347–353
Hérin E, Gardavaud F, Chiaradia M et al (2015) Use of Model-Based Iterative Reconstruction (MBIR) in reduced-dose CT for routine follow-up of patients with malignant lymphoma: dose savings, image quality and phantom study. Eur Radiol 25:2362–2370
International Commission on Radiation Units and Measurements (2012) ICRU Report No. 87: Radiation dose and image-quality assessment in computed tomography. J ICRU 12:1–149
Hsieh J (2009) Computed Tomography: principles, design, artifacts, and recent advances, 2nd edn. SPIE, Bellingham
Schneider CA, Rasband WS, Eliceiri KW (2012) NIH Image to ImageJ: 25 years of image analysis. Nat Methods 9:671–675
Rosset A, Spadola L, Ratib O (2004) OsiriX: an open-source software for navigating in multidimensional DICOM images. J Digit Imaging 17:205–216
International Electrotechnical Commission (2009), Medical electrical equipment - Part 2-44: Particular requirements for the basic safety and essential performance of X-ray equipment for computed tomography, IEC publication No. 60601-2-44
ICRP (2007) The 2007 Recommendations of the International Commission on Radiological Protection. ICRP publication 103. Ann ICRP 37
Bongartz G, Golding SJ, Jurik AG, et al. (2004) European Guidelines for Multislice Computed Tomography. European Commission, EUR 16262 EN
Shrimpton PC, Hillier MC, Lewis MA, Dunn M (2006) National survey of doses from CT in the UK: 2003. Br J Radiol 79:968–980
Menke J (2005) Comparison of different body size parameters for individual dose adaptation in body CT of adults. Radiology 236:565–571
Mitsumori LM, Shuman WP, Busey JM, Kolokythas O, Koprowicz KM (2012) Adaptive statistical iterative reconstruction versus filtered back projection in the same patient: 64 channel liver CT image quality and patient radiation dose. Eur Radiol 22:138–143
Fleischmann D, Boas FE (2011) Computed tomography - old ideas and new technology. Eur Radiol 21:510–517
Neeman Z, Dromi SA, Sarin S, Wood BJ (2006) CT fluoroscopy shielding: decreases in scattered radiation for the patient and operator. J Vasc Interv Radiol 17:1999–2004
Kato R, Katada K, Anno H, Suzuki S, Ida Y, Koga S (1996) Radiation dosimetry at CT fluoroscopy: physician's hand dose and development of needle holders. Radiology 201:576–578
Irie T, Kajitani M, Itai Y (2001) CT fluoroscopy-guided intervention: marked reduction of scattered radiation dose to the physician's hand by use of a lead plate and an improved I-I device. J Vasc Interv Radiol 12:1417–1421
Katada K, Kato R, Anno H et al (1996) Guidance with real-time CT fluoroscopy: early clinical experience. Radiology 200:851–856
Stoeckelhuber BM, Leibecke T, Schulz E et al (2005) Radiation dose to the radiologist's hand during continuous CT fluoroscopy-guided interventions. Cardiovasc Intervent Radiol 28:589–594
Mahnken AH, Sedlmair M, Ritter C, Banckwitz R, Flohr T (2012) Efficacy of lower-body shielding in computed tomography fluoroscopy-guided interventions. Cardiovasc Intervent Radiol 35:1475–1479
Hohl C, Suess C, Wildberger JE et al (2008) Dose reduction during CT fluoroscopy: phantom study of angular beam modulation. Radiology 246:519–525
Acknowledgements
We thank Toshiba Medical Systems Corporation for funding the clinical trial.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Jens Ricke.
Conflict of interest
The authors of this manuscript declare relationships with Toshiba Medical Systems Corporation.
Funding
This study has received funding by Toshiba Medical Systems Corporation.
Statistics and biometry
One of the authors has significant statistical expertise.
Ethical approval
Institutional Review Board approval was obtained.
Informed consent
Written informed consent was obtained from all subjects (patients) in this study.
Methodology
• retrospective
• observational
• performed at one institution
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOC 73 kb)
Rights and permissions
About this article

Cite this article
Grosser, O.S., Wybranski, C., Kupitz, D. et al. Improvement of image quality and dose management in CT fluoroscopy by iterative 3D image reconstruction. Eur Radiol 27, 3625–3634 (2017). https://doi.org/10.1007/s00330-017-4754-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-017-4754-7