
Abstract
Background
The number of elderly patients diagnosed with hepatocellular carcinoma (HCC) is progressively increasing. The aim of this study was to determine the safety and efficacy of conventional transarterial chemoembolization (TACE) in elderly HCC patients compared with younger adults.
Methods
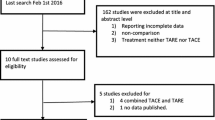
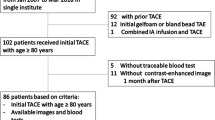
A consecutive cohort of unresectable HCC patients treated with TACE as a first-line treatment was retrospectively analyzed. Patients were categorized into “elderly” (≥ 70 years, 80 patients) and “younger” (< 70 years, 145 patients). Liver-related death and progression-free survival after TACE were compared before and after propensity score matching. A competing risk regression analysis was used for univariate/multivariate survival data analysis.
Results
cTACE was well tolerated in both groups. The cumulative risk of both liver-related death and progression-free survival after cTACE was comparable between “elderly” and “younger” (death: 73.8% vs 69.4%, P = 0.505; progression-free survival: 48.2% vs 44.8%, P = 0.0668). Propensity model matched 61 patients in each group for gender and Barcelona Clinic Liver Cancer staging. Even after matching, the cumulative risk of liver-related death and of progression-free survival did not differ between the two groups. At multivariate analysis, Child–Pugh class, tumor gross pathology and alpha-fetoprotein were independently associated with the liver-related mortality risk.
Conclusions
This study confirms that TACE is well tolerated and effective in patients aged 70 years or more with unresectable HCC as it is for their younger counterparts (< 70 years). Liver-related mortality was not associated with age ≥ 70 years and primarily predicted by tumor multifocality, Child–Pugh class B and an increased alpha-fetoprotein value (> 31 ng/ml).



Similar content being viewed by others

References
Liu Z, Jiang Y, Yuan H, Fang Q, Cai N, Suo C, Jin L, Zhang T, Chen X. The trends in incidence of primary liver cancer caused by specific etiologies: results from the global burden of disease study 2016 and implications for liver cancer prevention. J Hepatol. 2019;70:674–83.
Kulik L, El-Serag HB. Epidemiology and management of hepatocellular carcinoma. Gastroenterology. 2019;156:477–91.
White DL, Thrift AP, Kanwal F, Davila J, El-Serag HB. Incidence of hepatocellular carcinoma in all 50 United States, from 2000 through 2012. Gastroenterology. 2017;152:812–20.
Asahina Y, Tsuchiya K, Tamaki N, Hirayama I, Tanaka T, Sato M, Yasui Y, Hosokawa T, Ueda K, Kuzuya T, Nakanishi H, Itakura J, Takahashi Y, Kurosaki M, Enomoto N, Izumi N. Effect of aging on risk for hepatocellular carcinoma in chronic hepatitis C virus infection. Hepatology. 2010;52:518–27.
Cho SJ, Yoon JH, Hwang SS, Lee HS. Do young hepatocellular carcinoma patients with relatively good liver function have poorer outcomes than elderly patients? J Gastroenterol Hepatol. 2007;22:1226–311.
Borzio M, Fornari F, De Sio I, Andriulli A, Terracciano F, Parisi G, Francica G, Salvagnini M, Marignani M, Salmi A, Farinati F, Carella A, Pedicino C, Dionigi E, Fanigliulo L, Cazzaniga M, Ginanni B, Sacco R, EpaHCC Group. Adherence to American association for the study of liver diseases guidelines for the management of hepatocellular carcinoma: results of an Italian field practice multicenter study. Future Oncol. 2013;9:283–94.
Nordenstedt H, White DL, El-Serag HB. The changing pattern of epidemiology in hepatocellular carcinoma. Dig liver Dis. 2010;42(Suppl 3):S206–S214214.
Bucci L, Garuti F, Lenzi B, Pecorelli A, Farinati F, Giannini EG, Granito A, Ciccarese F, Rapaccini GL, Di Marco M, Caturelli E, Zoli M, Borzio F, Sacco R, Cammà C, Virdone R, Marra F, Felder M, Morisco F, Benvegnù L, Gasbarrini A, Svegliati-Baroni G, Foschi FG, Missale G, Masotto A, Nardone G, Colecchia A, Bernardi M, Trevisani F, Italian Liver Cancer (ITA.LI.CA) group. The evolutionary scenario of hepatocellular carcinoma in Italy: an update. Liver Int. 2017;37:259–70.
European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69:182–236.
Mirici-Cappa F, Gramenzi A, Santi V, Zambruni A, Di Micoli A, Frigerio M, Maraldi F, Di Nolfo MA, Del Poggio P, Benvegnù L, Rapaccini G, Farinati F, Zoli M, Borzio F, Giannini EG, Caturelli E, Bernardi M, Trevisani F, Italian Liver Cancer Group. Treatments for hepatocellular carcinoma in elderly patients are as effective as in younger patients: a 20-year multicentre experience. Gut. 2010;59:387–96.
Cohen MJ, Bloom AI, Barak O, Klimov A, Nesher T, Shouval D, Levi I, Shibolet O. Trans-arterial chemo-embolization is safe and effective for very elderly patients with hepatocellular carcinoma. World J Gastroenterol. 2013;19:2521–8.
Cohen MJ, Levy I, Barak O, Bloom AI, Fernández-Ruiz M, Di Maio M, Perrone F, Poon RT, Shouval D, Yau T, Shibolet O. Trans-arterial chemo-embolization is safe and effective for elderly advanced hepatocellular carcinoma patients: results from an international database. Liver Int. 2014;34:1109–17.
Nishikawa H, Kita R, Kimura T, Ohara Y, Takeda H, Sakamoto A, Saito S, Nishijima N, Nasu A, Komekado H, Osaki Y. Transcatheter arterial chemoembolization for intermediate-stage hepatocellular carcinoma: clinical outcome and safety in elderly patients. J Cancer. 2014;5:590–7.
Cheng HM, Tanaka T, Nishiofuku H, Chanoki Y, Horiuchi K, Masada T, Tatsumoto S, Matsumoto T, Marugami N, Kichikawa K. Safety and prognosis of transarterial chemoembolization for octogenarians with hepatocellular carcinoma. Cardiovasc Interv Radiol. 2019;42:1413–9.
Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30:52–60.
Trotti A, Colevas AD, Setser A, Rusch V, Jaques D, Budach V, Langer C, Murphy B, Cumberlin R, Coleman CN, Rubin P. CTCAE v3.0: development of a comprehensive grading system for the adverse effects of cancer treatment. Semin Radiat Oncol. 2003;13:176–81.
Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc. 1999;94:496–509.
Gray RJ. A class of K-sample tests for comparing the cumulative incidence of a competing risk. Ann Stat. 1988;16:1141–54.
D’Agostino RB Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non randomized control group. Stat Med. 1998;17:2265–81.
Putter H, Fiocco M, Geskus RB. Tutorial in biostatistics: competing risks and multi-state models. Stat Med. 2007;26:2389–430.
Mondazzi L, Bottelli R, Brambilla G, Rampoldi A, Rezakovic I, Zavaglia C, Alberti A, Idèo G. Transarterial oily chemoembolization for the treatment of hepatocellular carcinoma: a multivariate analysis of prognostic factors. Hepatology. 1994;19:1115–23.
Biselli M, Forti P, Mucci F, Foschi FG, Marsigli L, Caputo F, Ravaglia G, Bernardi M, Stefanini GF. Chemoembolization versus chemotherapy in elderly patients with unresectable hepatocellular carcinoma and contrast uptake as prognostic factor. J Gerontol A Biol Sci Med Sci. 1997;52:305–9.
Fujii H, Itoh Y, Ohnishi N, Sakamoto M, Ohkawara T, Sawa Y, Nishida K, Ohkawara Y, Yamaguchi K, Minami M, Okanoue T. Factors associated with the overall survival of elderly patients with hepatocellular carcinoma. World J Gastroenterol. 2012;18:1926–32.
Yau T, Yao TJ, Chan P, Epstein RJ, Ng KK, Chok SH, Cheung TT, Fan ST, Poon RT. The outcomes of elderly patients with hepatocellular carcinoma treated with transarterial chemoembolization. Cancer. 2009;115:5507–15.
Lee SH, Choi HC, Jeong SH, Lee SH, Choi HC, Jeong SH, Lee KH, Chung JI, Park YS, Hwang JH, Kim JW, Kim N, Lee DH, et al. Hepatocellular carcinoma in older adults: clinical features, treatments, and survival. J Am Geriatr Soc. 2011;59:241–50.
Nomura F, Ohnishi K, Honda M, Satomura Y, Nakai T, Okuda K. Clinical features of hepatocellular carcinoma in the elderly: a study of 91 patients older than 70 years. Br J Cancer. 1994;70:690–3.
Poon RT, Fan ST, Lo CM, Liu CL, Ngan H, Ng IO, Wong J. Hepatocellular carcinoma in the elderly: results of surgical and nonsurgical management. Am J Gastroenterol. 1999;94:2460–6.
Funding
This study was not supported by any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed Consent
For this type of study formal consent is not required. Informed consent was obtained from all individual participants included in the study.
Consent for Publication
For this type of study consent for publication is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Mosconi, C., Gramenzi, A., Biselli, M. et al. Survival and Tolerability of Transarterial Chemoembolization in Greater Versus less than 70 Years of Age Patients with Unresectable Hepatocellular Carcinoma: A Propensity Score Analysis. Cardiovasc Intervent Radiol 43, 1015–1024 (2020). https://doi.org/10.1007/s00270-020-02451-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-020-02451-3