
Abstract
Purpose
We present findings concerning 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET) at end-treatment evaluation in follicular lymphoma (FL) in order to establish possible predictive factors for progression-free survival (PFS) and patient outcome.
Methods
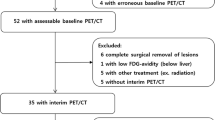
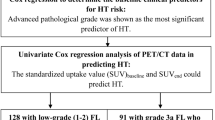
We retrospectively analysed data from 91 consecutive FL patients (M:F = 51:40, mean age 61) referred to our PET Unit at therapy completion: 38 with an indolent form (grade 1–2) and 53 with an aggressive FL (grade 3a and b) according to the World Health Organization (WHO) classification. A total of 148 FDG PET/CT scans were analysed and findings reported as positive or negative for disease. The overall response to treatment was assessed according to the revised International Workshop Criteria (IWC). The final outcome was defined as remission or disease by taking clinical, instrumental and histological data as standards of reference, with a mean follow-up period of 3 years (range 1–8). A statistical analysis was performed with respect to PFS and patient outcome for FDG PET result, tumour grading, Follicular Lymphoma International Prognostic Index (FLIPI), disease stage and number of relapses, on uni- and multivariate analyses, with p < 0.05 considered as significant.
Results
Overall patients presented a mean PFS of 35 months (range 3–86), with a relapse rate of 42%. At final outcome, remission was achieved in 67 of 91 patients (74%). Of the different predictive factors, only FDG PET result significantly correlated with patient outcome (p = 0.0002). PET/CT performance at the end of treatment was as follows: 100% sensitivity, 99% specificity, 89% positive predictive value and 100% negative predictive value. The Kaplan-Meier analysis demonstrated a statistically significant correlation with PFS for FDG PET (p < 0.0001), FLIPI score (0–1 versus ≥2) (p = 0.0451) and number of relapses (none versus ≥1) (p = 0.0058). These findings were confirmed at the univariate analysis, whereas at the multivariate analysis only FDG PET (p = 0.0006892) and number of relapses (p = 0.01947) were independent predictive factors for PFS.
Conclusion
End-treatment PET/CT in FL has high accuracy and appears to be a good predictor of PFS and patient outcome, irrespective of grading. As expected, patients facing more than one relapse seem to have significantly shorter PFS in the presence of a positive FDG PET.



Similar content being viewed by others

References
Armitage JO, Weisenburger DD. New approach to classifying non-Hodgkin’s lymphomas: clinical features of the major histologic subtypes. Non-Hodgkin’s Lymphoma Classification Project. J Clin Oncol 1998;16:2780–95.
Bartlett NL, Witzig TE, Gordon L, Beck T, Fehrenbacher L, Kommehl E, et al: 90Y-ibritumomab tiuxetan (Zevalin) radioimmunotherapy for transformed B-cell non-Hodgkin’s lymphoma (NHL) patients. ASCO Annual Meeting. Proc Am Soc Clin Oncol 2002;21:Abstract 51.
Nathwani BN, Harris NL, Weisenburger D, et al. Follicular lymphoma. In: Jaffe ES, Harris NL, Stein H, Vardiman JW, editors. WHO classification of tumours. Pathology and genetics of tumours of haematopoietic and lymphoid tissues. Lyon: IARC Press; 2001. p. 162–7.
Solal-Céligny P, Roy P, Colombat P, White J, Armitage JO, Arranz-Saez R, et al. Follicular lymphoma international prognostic index. Blood 2004;104:1258–65.
Jacene HA, Filice R, Kasecamp W, Wahl RL. 18F-FDG PET/CT for monitoring the response of lymphoma to radioimmunotherapy. J Nucl Med 2009;50(1):8–17.
Cheson BD, Pfistner B, Juweid ME, Gascoyne RD, Specht L, Horning SJ, et al. Revised response criteria for malignant lymphoma. J Clin Oncol 2007;25:579–86.
Spaepen K, Stroobants S, Dupont P, Thomas J, Vandenberghe P, Balzanini J, et al. Can positron emission tomography with [(18)F]-fluorodeoxyglucose after first-line treatment distinguish Hodgkin’s disease patients who need additional therapy from others in whom additional therapy would mean avoidable toxicity? Br J Haematol 2001;115:272–8.
Zinzani PL, Fanti S, Battista G, Tani M, Castellucci P, Stefoni V, et al. Predictive role of positron emission tomography (PET) in the outcome of lymphoma patients. Br J Cancer 2004;91:850–4.
Reinhardt MJ, Herkel C, Altehoefer C, Finke J, Moser E. Computed tomography and 18F-FDG positron emission tomography for therapy control of Hodgkin’s and non-Hodgkin’s lymphoma patients: when do we really need FDG-PET? Ann Oncol 2005;16:1524–9.
Le Dortz L, De Guibert S, Bayat S, Devillers A, Houot R, Rolland Y, et al. Diagnostic and prognostic impact of 18F-FDG PET/CT in follicular lymphoma. Eur J Nucl Med Mol Imaging 2010;37:2307–14.
Bishu S, Quigley JM, Bishu SR, Olsasky SM, Stem RA, Shostrom VK, et al. Predictive value and diagnostic accuracy of F-18-fluoro-deoxy-glucose positron emission tomography treated grade 1 and 2 follicular lymphoma. Leuk Lymphoma 2007;48:1548–55.
Zinzani PL, Musuraca G, Alinari L, Fanti S, Tani M, Stefoni V, et al. Predictive role of positron emission tomography in the outcome of patients with follicular lymphoma. Clin Lymphoma Myeloma 2007;7:291–5.
Elstrom R, Guan L, Baker G, Nakhoda K, Vergilio JA, Zhuang H, et al. Utility of FDG-PET scanning in lymphoma by WHO classification. Blood 2003;101:3875–387.
Tsukamoto N, Kojima M, Hasegawa M, Oriuchi N, Matsushima T, Yokohama A, et al. The usefulness of (18)F-fluorodeoxyglucose positron emission tomography ((18)F-FDG-PET) and a comparison of (18)F-FDG-PET with (67)gallium scintigraphy in the evaluation with lymphoma: relation to histologic subtypes based on the World Health Organization classification. Cancer 2007;110(3):652–9.
Karam M, Novak L, Cyriac J, Ali A, Nazeer T, Nugent F. Role of fluorine-18 fluoro-deoxyglucose positron emission tomography scan in the evaluation and follow-up of patients with low-grade lymphomas. Cancer 2006;107:175–83.
Weiler-Sagie M, Bushelev O, Epelbaum R, Dann EJ, Haim N, Avivi L, et al. (18)F-FDG avidity in lymphoma readdressed: a study of 766 patients. J Nucl Med 2010;51:25–30.
Wöhrer S, Jaeger U, Kletter K, Becherer A, Hauswirth A, Turetschek K, et al: 18F-fluoro-deoxy-glucose positron emission tomography (18F-FDG-PET) visualizes follicular lymphoma irrespective of grading. Ann Oncol 2006;17:780–4.
Jerusalem G, Beguin Y, Najjar F, Hustinx R, Fassotte MF, Rigo P, et al. Positron emission tomography (PET) with 18F-fluorodeoxyglucose (18F-FDG) for the staging of low-grade non-Hodgkin’s lymphoma (NHL). Ann Oncol 2001;12(6):825–30.
Hicks RJ. The role of PET in monitoring therapy. Cancer Imaging 2005;5:51–7.
Young H, Baum R, Cremerius U, Herholz K, Hoekstra O, Lammertsma AA, et al. Measurement of clinical and subclinical tumour response using [18F]-fluorodeoxyglucose and positron emission tomography: review and 1999 EORTC recommendations. European Organization for Research and Treatment of Cancer (EORTC) PET Study Group. Eur J Cancer 1999;35:1773–82.
Harris NL, Jaffe ES, Diebold J, Flandrin G, Muller-Hermelink HK, Vardiman J, et al. World Health Organization classification of neoplastic diseases of the hematopoietic and lymphoid tissues: report of the Clinical Advisory Committee Meeting, Airlie House, Virginia, November 1997. J Clin Oncol 1999; 17:3835–49.
Carbone PP, Kaplan HS, Musshoff K, Smithers DW, Tubiana M. Report of the Committee on Hodgkin’s Disease Staging Classification. Cancer Res 1971;31:1860–1.
Zinzani PL, Stefoni V, Tani M, Fanti S, Musuraca G, Castellucci P, et al. Role of [18F]fluorodeoxyglucose positron emission tomography scan in the follow-up of lymphoma. J Clin Oncol 2009;27(11):1781–7.
Hutchings M, Specht L. PET/CT in the management of haematological malignancies. Eur J Haematol 2008;80(5):369–80.
Cheson BD, Horning SJ, Coiffier B, Shipp MA, Fisher RI, Connors JM, et al. Report of a international workshop to standardize response criteria for non-Hodgkin’s lymphomas. NCI Sponsored International Working Group. J Clin Oncol 1999;17:1244–53.
Shöder H, Noy A, Gönen M, Weng L, Green D, Erdi YE, et al. Intensity of 18fluorodeoxyglucose uptake in positron emission tomography distinguishes between indolent and aggressive non-Hodgkin’s lymphoma. J Clin Oncol 2005;23:4643–51.
Watanabe R, Tomita N, Takeuchi K, Sakata S, Tateishi U, Tanaka M, et al. SUVmax in FDG-PET at the biopsy site correlates with the proliferation potential of tumor cells in non-Hodgkin lymphoma. Leuk Lymphoma 2010;51(2):279–83.
Najjar F, Hustinx R, Jerusalem G, Filet G, Rigo P. Positron emission tomography (PET) for staging low-grade non-Hodgkin’s lymphomas (NHL). Cancer Biother Radiopharm 2001;16(4):297–304.
Lopci E, Santi I, Derenzini E, Fonti C, Savelli G, Bertagna F, et al. FDG-PET in the assessment of patients with follicular lymphoma treated by ibritumomab tiuxetan Y90: multicentric study. Ann Oncol 2010;21:1877–83.
Imataki O, Tamai Y, Yokoe K, Furukawa T, Kawakami K. The utility of FDG-PET for managing patients with malignant lymphoma: analysis of data from a single cancer center. Intern Med 2009;48:1509–13.
Blum RH, Seymur JF, Wirth A, MacManus M, Hicks RJ. Frequent impact of [18F]fluorodeoxyglucose positron emission tomography on the staging and management of patients with indolent non-Hodgkin’s lymphoma. Clin Lymphoma 2003;4:43–9.
Wirth A, Foo M, Seymur JF, MacManus MP, Hicks RJ. Impact of [18F] fluorodeoxyglucose positron emission tomography on staging and management of early-stage follicular non-Hodgkin lymphoma. Int J Radiat Oncol Biol Phys 2008;71(1):213–9.
Trotman J, Fournier M, Lamy T, Seymour JF, Sonet A, Jankova A, et al. Positron emission tomography-computed tomography (PET-CT) after induction therapy is highly predictive of patient outcome in follicular lymphoma: analysis of PET-CT in a subset of PRIMA trial participants. J Clin Oncol 2011;29:3194–200.
Author information
Authors and Affiliations
Corresponding author
Additional information
E. Lopci and L. Zanoni contributed equally to this paper.
Rights and permissions
About this article
Cite this article
Lopci, E., Zanoni, L., Chiti, A. et al. FDG PET/CT predictive role in follicular lymphoma. Eur J Nucl Med Mol Imaging 39, 864–871 (2012). https://doi.org/10.1007/s00259-012-2079-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-012-2079-y