
Abstract
Objective
To evaluate the feasibility of hand MRI in age assessment in adolescents using the Greulich-Pyle (GP) atlas criteria.
Materials and methods
Two radiologists, who were blinded to the study subjects’ chronologic ages, semi-objectively evaluated 1.5-T MRIs of the left hands of ten patients (13.5 ± 2.6 years) who had left-hand radiographs and 50 healthy volunteers (15 ± 2 years).
Results
A coronal T1-weighted, volumetric, interpolated, breath-hold examination with water excitation (T1 VIBE-3D-WE) achieved the best image quality. The correlation between estimated patients’ ages on radiographs and MRI was high. The average estimated age difference between the MRIs and radiographs was −0.05 years for reader 1 and −0.175 years for reader 2. The interclass coefficients (ICCs) showed high interobserver agreement (radiographs: ICC = 0.95, MRI: ICC = 0.97). The ICC, calculated separately for the male and female volunteers’ estimated ages by MRI, also showed a high agreement between the two readers (male: ICC = 0.97, female: ICC = 0.95). Reader 1 estimated 94% of volunteers within 2 standard deviations (SD) and 62% within 1 SD. The results for reader 2 were 92% and 54%, respectively. Thirty-nine percent of girls and 27% of boys were estimated to be older using 1 SD.
Conclusion
MRI of the left hand is a feasible alternative to hand radiographs for skeletal age estimation in adolescents using the GP criteria with 2 SD. Using 1 SD, the age of healthy volunteers tended to be estimated as higher than the chronologic age. Future studies should evaluate the results in a larger number of participants.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Since Heinrich von Ranke introduced the use of the hand X-ray to evaluate pediatric growth in 1896, this method has become an important tool in the assessment of the normal and pathologic development of children [1]. Skeletal maturity assessment is clinically essential for pediatric orthopedics in preoperative planning [1, 2], for the diagnosis and treatment of pediatric growth development failure due to congenital or iatrogenic endocrinologic disorders or after chemotherapy or radiation therapy of oncologic patients [3,4,5,6,7]. Repeated annual follow-up hand X-rays (0.0005 mSv effective dose per radiograph) [8], however, result in a not negligible cumulative radiation dose. This method has also been used for forensic age estimation in living individuals [9, 10]. Magnetic resonance imaging (MRI) of the left hand has been preliminarily tested for the assessment of bone maturation [11,12,13,14,15,16]. Only one pilot study correlated the age estimated by MRI with a radiograph of the left hand [16].
The aim of our study was to evaluate the feasibility of MRI of the left hand to replace the standard radiograph of the left hand in age estimation based on the Greulich-Pyle (GP) hand atlas criteria as the reference standard. The first part of the study aimed to analyze various MR sequences to select the optimal sequence for age estimation and to assess the reliability of MRI of the left hand for skeletal age estimation compared with a standard radiograph of the left hand of patients; the second part aimed to compare the age estimated by MRI with the chronologic age of volunteers.
Methods and materials
Patients and healthy volunteers
The local ethics committee approved this prospective study. Written informed consent was obtained from all patients and volunteers or from their parents if they were minors.
Inclusion criteria were informed consent, lack of either MRI contraindications or need of sedation, and furthermore, for volunteers, no past medical history of any chronic diseases. The exclusion criterion was noncompliance during the examination.
In the first part of the study, ten patients (eight males and two females; mean age, 13.5 years; range, 11–18 years) with endocrinologic diseases, in whom a standard radiograph of the left hand had been performed, also underwent an MRI of the left hand within a week of the radiograph. All of the patients were native Europeans (at least two generations of ancestors born in Europe).
In the second part of the study, 50 healthy volunteers (17 males and 33 females; mean age, 15 years; range, 12–19.8 years) underwent an MRI of the left hand. All healthy volunteers were middle-class and born in Europe. Forty-six healthy volunteers were native Europeans (at least two generations of ancestors born in Europe), and the parents of the remaining four volunteers were from Iran, Argentina, Mali, and the Philippines.
Imaging technique
All radiographs of the left hand in the first part of the study were performed in the dorsovolar projection on an X-ray unit (Polydoros IT Opti 150/12/50 C®, Siemens Healthineers, Siemens Healthcare GmbH, Germany) using 18 × 24-cm Fuji storage phosphor plates and a Fuji Dry Laser machine (Fuji DryPix 7000®, Fujifilm Holdings Corp., Tokyo, Japan).
All MRI examinations were performed on a short 1.5-T closed-bore (bore size 60-cm) scanner (Magnetom Avanto®, Siemens Healthineers, Siemens Healthcare GmbH, Germany), using a head-neck coil combination and in the prone position with the left arm outstretched (superman position). To reduce motion artifacts, a small sandbag was placed on the left hand.
In the first part of the study, three sequences were applied:
-
(1)
Coronal T1-weighted turbo-inversion recovery magnitude (T1 TIRM):
-
a.
Matrix: 176 × 384; voxel size: 0.5 × 0.5 × 3.0 mm; field of view (FOV): 200 mm; slice thickness (SL): 3 mm; gap: 0.3 mm; repetition time (TR): 4110 ms; echo time (TE): 47 ms; inversion time: 150 ms; flip angle: 150°; acquisition time: 3 min and 31 sec
-
a.
-
(2)
Coronal T1-weighted volumetric interpolated breath-hold examination with water excitation (T1 VIBE-3D-WE):
-
a.
Matrix: 384 × 512; voxel size: 0.4 × 0.4 × 1.5 mm; FOV: 230 mm; SL: 1.5; gap: 0.3 mm; TR: 14.6 ms; TE: 6.07 ms; flip angle: 15°; acquisition time: 2 min and 26 sec
-
a.
-
(3)
Coronal T1-weighted spin echo (T1 SE):
-
a.
Matrix: 384 × 512; voxel size: 0.4 × 0.4 × 2.0 mm; FOV: 200 mm; SL: 2 mm; gap: 0.2 mm; TR: 523 ms; TE: 23 ms; flip angle: 90°; acquisition time: 5 min and 5 sec
-
a.
In the second part of the study, only the coronal T1 VIBE-3D-WE sequence was applied, with the same parameters as described above.
The MRI software version “Syngo MR B13 4VB13A” (Siemens Healthineers, Siemens Healthcare GmbH, Germany) was used in the first part of the study and “Syngo MR B17” (Siemens Healthineers, Siemens Healthcare GmbH, Germany) in the second part.
Evaluation
Two radiologists with 9 (consultant pediatric radiologist, reader 1) and 20 years (senior consultant musculoskeletal radiologist) of experience in musculoskeletal radiology evaluated the three sequences and determined the image quality and usefulness for the assessment of bone maturation parameters using a 10-point scale.
The decision criteria were:
-
(1)
Ossification recognition, defined as the delineation of ossified and cartilaginous parts versus joint spaces
-
(2)
Diagnostic usefulness, defined as the contrast between the ossified and cartilaginous matrix
-
(3)
Overall subjective image quality
-
(4)
Motion and other artifacts
The image quality was rated as 1–2 for non-diagnostic, 3–4 for poor, 5–6 for acceptable, 7–8 for good, and 9–10 for excellent quality. For artifacts, the 10-step scale defined 1–2 as non-diagnostic, 3–4 as severe, 5–6 as moderate, 7–8 as mild artifacts, and 9–10 as an absence of artifacts.
Mean values were calculated for all evaluated parameters and the sequence considered the best was used for age estimation in the first and second parts of the study.
In addition, two consultant radiologists with 9 (consultant pediatric radiologist, reader 1) and 8 years (consultant musculoskeletal radiologist, reader 2) of experience in skeletal age estimation performed semiquantitative subjective age estimation on all images, blinded to the chronologic age of the volunteers and patients, based on the parameters of the GP atlas.
All study images were assessed on a picture-archiving and communication system (PACS) station (IMPAX ES, DS 3000©, Agfa Healthcare, Mortsel, Belgium).
In the first part of the study, the readers reviewed the radiographs of the patients’ left hands, and, after a 1-month time interval, the readers reviewed the MRIs of the left hands of these patients using the most useful MRI sequence and then independently determined an estimated age for each patient and each examination.
The evaluation criteria for age estimation were the ossification stages of the epiphysis of the radius and ulna, carpal bones, metacarpal bones, thumb extensor and flexor sesamoid, and phalanges.
In the second part of the study, the two readers reviewed the MRIs of the left hands of healthy volunteers using the same evaluation criteria as in the first part of the study and independently estimated the skeletal age of each volunteer. In addition, males and females were analyzed separately.
Statistical analysis
Bland-Altman plots [17] for both readers were drawn for the ten patients to determine agreement between radiographs and MRIs. Estimates for the mean difference between radiographs and MRIs and for the 95% limits of agreement (defined as the mean difference ± 1.96 SD of the difference) were calculated. For all estimates, 95% confidence intervals (CI) were calculated. Intraclass correlation coefficients (ICC) were calculated for radiographs and for MRIs to determine agreement between readers 1 and 2.
For the age estimation of the healthy volunteers, Bland-Altman analysis for both readers was performed for males and females separately. The standard deviation in the Greulich-Pyle atlas is provided only up until 17 years (boys) and 15 years of age (girls). For volunteers outside that range, the last available standard deviation was assumed. ICCs were also calculated for male and female volunteers separately to determine agreement between the readers in both groups.
Results
All examinations were well tolerated and completed with no compliance issues.
Comparison of the three different sequences by subjective evaluation revealed the best values for the coronal T1 VIBE-3D-WE, including visibility of the anatomic structures (Table 1 and Fig. 1a and b). As T1 VIBE-3D-WE was also the shortest sequence (acquisition time 2 min and 26 sec), it was chosen for age estimation for the first and second parts of the study.

(a) Radiograph of the left hand and (b) coronal T1 SE, T1 TIRM, and T1 VIBE-3D-WE (from left to right) of an 11-year-old male with growth failure. The image quality of T1 VIBE-3D-WE was evaluated as better than the other sequences
In the first part of the study, the comparison of age estimation by radiographs and MRIs revealed a high correlation between these methods (Table 2). The Bland-Altman plots for both readers are provided in Fig. 2a and b.

a and b The Bland-Altman plots for both readers in the first part of the study. The plots show the mean of the estimated ages from the two methods (radiographs and MRIs) on the x-axis, given in years, and the difference between the estimated ages on the y-axis, also given in years. The dotted lines give 95% limits of agreement for estimated ages (average difference ± 1.96 SD of the difference)
The Bland-Altman plot for reader 1 shows that the estimated ages with MRIs and radiographs matched in seven children. The average age difference between MRIs and radiographs was −0.05 years (95% CI: -0.60; 0.40), and the limits of agreement ranged from −1.54 years (95% CI: -2.08; −1) to 1.44 years (95% CI: 0.90; 1.98). Only one patient was estimated to be 2 years older by the MRI compared with the radiograph. For reader 2, the differences between estimated ages by MRI and radiograph were ± 1 year. The average age difference was −0.175 years (95% CI: -0.57; 0.22), and, compared with reader 1, the range of the limits of agreement was narrower, from −1.26 years (95% CI: -1.65; −0.87) to 0.91 years (95% CI: 0.52; 1.30).
It was expected that 95% of the differences would lie between these limits. As the range of the limits of agreement is not clinically important, the two methods can be used interchangeably [17]. ICC showed a high agreement for the two readers: 0.95 for radiographs and 0.97 for MRIs.
In the second part of the study, a comparison of the estimated age by hand MRI with the true chronologic age of the healthy male and female volunteers was made, and the results are presented in Table 3.
The Bland-Altman plots for both readers are given in Fig. 3a–d (for males: Fig. 3a and c and for females: Fig. 3b and d).

a–d The Bland-Altman plots for both readers in the second part of the study for (a) males and (b) females for reader 1 and for (c) males and (d) females for reader 2. The chronologic age of the volunteers is shown on the x-axis and the differences between the assessed age and chronologic age on the y-axis, given in years. The dotted lines correspond to 95% limits of agreement. The continuous lines present the 1st and 2nd SD related to the volunteers’ ages
Of the 15 male volunteers in the age group where the standard deviation (SD) was available in the GP atlas, 11 (73%) and 8 (53%) were estimated correctly within 1 SD, and 15 (100%) and 14 (93%) were estimated correctly within 2 SD by reader 1 and reader 2, respectively. The two male volunteers with a chronologic age of 18 years or older were estimated at 19 years of ages by both readers. Of the 22 female volunteers in the age group where the SD was available in the GP atlas, 12 (55%) were estimated correctly within 1 SD, and 20 (91%) were estimated correctly within 2 SD by both readers. The three female volunteers with a chronologic age of 18 years or greater were all estimated at 18 years of age by reader 1, and only one of the three was estimated at 17 years of age by reader 2.
Using 1 SD, the ages of nine females (41%) were estimated to be older than their chronologic ages, and the age of only one female (5%) was estimated to be younger than her chronologic age by reader 1. Reader 2 estimated eight females (36%) to be older than their chronologic age und two females (9%) younger than their chronologic age. Four males (27%) were estimated to be older than their chronologic age by both readers. No males were assessed younger than their chronologic ages by either reader.
We did not find any consistent bias for adjusting the estimated ages by MRI (Fig. 3a–d).
The ICC, calculated separately for males and females, also showed high agreement between the two readers for both groups (males: ICC = 0.97; females: ICC = 0.95).
The MR images of two healthy volunteers are presented in Figs. 4 and 5.

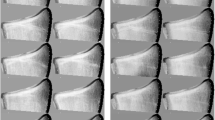
Four slices of a coronal T1 VIBE-3D-WE hand MRI of a 16-year-old healthy female. Estimated age was 18 years (reader 1) and 18 years (reader 2)

Two slices of a coronal T1 VIBE-3D-WE hand MRI of a 16-year-old healthy male. Estimated age was 17 years (reader 1) and 17 years (reader 2)
Discussion
In our study, we estimated the bone age by MRI and a radiograph of the left hand in accordance with GP criteria. In skeletal age estimation, a radiograph of the left hand is chosen rather than of the right hand, because the number of right-handed persons in most populations is much larger than that of left-handed individuals; consequently, the left hand is less likely to be injured than the hand that is used more frequently [18]. Dreizen et al. compared radiographs of left and right hands and stated that the divergences of the skeletal maturations of the two hands are negligible in the evaluation of skeletal status [19]. Roche found that the left hand was more advanced than the right hand [20], while Baer and Djrkatz found no such effect [21]. An automated age estimation of the metacarpals found no significant difference between the two sides [22].
Subjective systematic evaluation of three optimized high-resolution sequences (T1 TIRM, T1 VIBE-3D-WE, T1 SE) by two consultant radiologists with different years of experience revealed the best values for the coronal T1 VIBE-3D-WE, including visibility of the anatomic structures. It was also the shortest sequence. Short examination times are beneficial to avoid motion artifacts and maintain the compliance of children. Semiquantitative bone age estimation through the assessment of all anatomic landmarks was possible in all 60 subjects of our study with high interobserver agreement at 1.5 T using a single high-resolution T1 VIBE-3D-WE sequence and a head-neck coil combination.
Compared with the fast, low-angle shot three-dimensional fat-suppressed (FLASH 3D–FS) sequence, fat-suppressed 3D VIBE achieved images with a higher cartilage signal-to-noise ratio (SNR), higher contrast-to-noise ratio (CNR) between the cartilage and the surrounding tissues, and reduced pulsation artifacts in a much shorter acquisition time [23].
Tomei et al. used a low-field open magnet (0.2 T) with a hand and wrist coil and applied a coronal single T1 SE sequence with a scan time of 1 min 39 s [11]. Terada et al. also used a low-field (0.3-T) open compact magnet system and applied a 3D gradient echo (GRE) sequence, with a scan time of 2 min 44 s [14]. The choice of the magnet, however, depends on the availability within the environment. We used the 1.5-T short closed-bore magnet, which is used for diagnostic imaging in daily clinical practice, for both adults and children. In general, high-field closed-bore (1.5-T) MR scanners provide higher spatial and contrast resolution than do open low-field (0.2-T) scanners [24] and have revealed considerably higher image quality with less image noise as well as a higher SNR with a shorter scanning time [25].
We also found high agreement between the estimated bone ages using the coronal T1 VIBE-3D-WE of the left hand and the dorsovolar hand X-ray, based on the criteria of the GP atlas, for both consultant radiologists.
This is in contrast to George et al., who compared the fusion grades of the left wrist distal radial growth plate between MRIs and radiographs [15]. In their study, the bone age of 15–19-year-old male football players was estimated as higher with radiographs compared with MRIs [15]. However, the study focused on the radial growth plate of the left wrist and a single criterion only and used a coronal T1-weighted sequence [15]. Urschler et al. compared the estimated ages in 18 subjects using radiographs and MRIs of the left hand and stated that, in subjects between 14 and 18 years of age, the estimated ages by MRI were slightly lower than on a radiograph [16]. A possible explanation for these differences could be that the growth plate is better visible on cross-sectional imaging, such as MRI, than in projection radiographs. In the first part of our study, the average difference between estimated ages by MRI and a radiograph was not significant.
In the second part of the study, we also found high interobserver agreement for age estimation in healthy boys and girls using the coronal T1 VIBE-3D-WE of the left hand based on the GP criteria. This is in accordance with Tomei et al., who used a single T1 SE sequence [11]. We used the GP criteria, as this standard has been proven superior to Tanner and Whitehouse in terms of the time required to determine skeletal age and thus has been recommended for routine clinical practice [1]. The GP criteria also provide high interobserver agreement for age estimation for hand X-rays and hand MRIs compared with those of Tanner and Whitehouse [16].
We also observed that more than 90% of estimated bone ages for healthy volunteers (males and females) were within 2 SD (94% for reader 1 and 92% for reader 2). This corresponds to the GP atlas results using hand X-rays [18]. However, using 1 SD, our results (62% for reader 1 and 54% for reader 2) differed from the GP atlas results for hand X-rays, in which approximately two-thirds of the estimated ages were within 1 SD [18]. Although our volunteers were from the socioeconomic middle class with a background of good medical care, similar to those assessed by the GP atlas, which comprised X-rays of healthy white children, we also found that in the age group with an available SD, healthy volunteers also tended to be estimated as older than their chronologic age using 1 SD. As an overestimation of skeletal maturation would have implications for legal and medical procedures, such as in the diagnosis and treatment of growth failure, further studies with a larger number of study subjects should be performed.
The difference between our results and the GP results using 1 SD is likely attributable to skeletal maturation changes since 1950, reflecting the different standard deviations compared with the GP atlas, but may also be influenced by the small number of cases in our study. To our knowledge, there are no published data that address skeletal maturation changes from 1950 to the present at this time. Future studies should evaluate the results in a larger number of participants.
Study limitations
Our results were based on a small number of cases and focused also on children older than 10 years, who were cooperative during the examination, without any sedation. No comparison of ethnicities was performed. The gender distribution was asymmetric in both parts of the study. However, because the evaluation of boys and girls was performed separately, the results of the study should not be biased. Multicenter studies are necessary to confirm the study statements in a larger number of participants.
Conclusion
In conclusion, MRI of the left hand, using a single coronal sequence, T1 VIBE-3D-WE, in a routine scanner is a radiation-free alternative method feasible for skeletal age estimation of adolescents using the GP-based criteria. The age of healthy adolescents could be correctly estimated by expert readers within 2 SD by hand MRI and the Greulich-Pyle atlas, with high agreement. However, when using only 1 SD, bone ages tend to be estimated as older than the chronologic ages. Future studies should evaluate the results in a larger number of participants.
References
Horter MJ, Friesen S, Wacker S, Vogt B, Leidiger B, Roedl R, et al. Determination of skeletal age : comparison of the methods of Greulich and Pyle and Tanner and Whitehouse. Der Orthopade. 2012;41(12):966–76.
Sabharwal S, Sakamoto SM, Zhao C. Advanced bone age in children with Blount disease: a case-control study. J Pediatr Orthop. 2013;33(5):551–7.
Heuschkel R, Salvestrini C, Beattie RM, Hildebrand H, Walters T, Griffiths A. Guidelines for the management of growth failure in childhood inflammatory bowel disease. Inflamm Bowel Dis. 2008;14(6):839–49.
Even L, Andersson B, Kristrom B, Albertsson-Wikland K, Hochberg Z. Role of growth hormone in enchondroplasia and chondral osteogenesis: evaluation by X-ray of the hand. Pediatr Res. 2014;76(1):109–14.
Darendeliler F, Ranke MB, Bakker B, Lindberg A, Cowell CT, Albertsson-Wikland K, et al. Bone age progression during the first year of growth hormone therapy in pre-pubertal children with idiopathic growth hormone deficiency, Turner syndrome or idiopathic short stature, and in short children born small for gestational age: analysis of data from KIGS (Pfizer international growth database). Horm Res. 2005;63(1):40–7.
Bree AF, Siegfried EC. Acne vulgaris in preadolescent children: recommendations for evaluation. Pediatr Dermatol. 2014;31(1):27–32.
Lazar L, Phillip M. Pubertal disorders and bone maturation. Endocrinol Metab Clin N Am. 2012;41(4):805–25.
Hart D, Wall BF. NRPB-W4 Radiation Exposure of the UK Population from Medical and Dental X-ray Examinations. NRPB-W. National Radiological Protection Board: National Radiological Protection Board 2002.
Schmeling A, Dettmeyer R, Rudolf E, Vieth V, Geserick G. Forensic age estimation. Dtsch Arztebl Int. 2016;113(4):44–50.
Sauer PJ, Nicholson A, Neubauer D. Age determination in asylum seekers: physicians should not be implicated. Eur J Pediatr. 2016;175(3):299–303.
Tomei E, Sartori A, Nissman D, Al Ansari N, Battisti S, Rubini A, et al. Value of MRI of the hand and the wrist in evaluation of bone age: preliminary results. J Magn Reson Imaging : JMRI. 2014;39(5):1198–205.
Dvorak J, George J, Junge A, Hodler J. Age determination by magnetic resonance imaging of the wrist in adolescent male football players. Br J Sports Med. 2007;41(1):45–52.
Dvorak J, George J, Junge A, Hodler J. Application of MRI of the wrist for age determination in international U-17 soccer competitions. Br J Sports Med. 2007;41(8):497–500.
Terada Y, Kono S, Tamada D, Uchiumi T, Kose K, Miyagi R, et al. Skeletal age assessment in children using an open compact MRI system. Magnetic resonance in medicine: official journal of the Society of Magnetic Resonance in medicine. Magn Reson Med. 2013;69(6):1697–702.
George J, Nagendran J, Azmi K. Comparison study of growth plate fusion using MRI versus plain radiographs as used in age determination for exclusion of overaged football players. Br J Sports Med. 2012;46(4):273–8.
Urschler M, Krauskopf A, Widek T, Sorantin E, Ehammer T, Borkenstein M, et al. Applicability of Greulich-Pyle and Tanner-Whitehouse grading methods to MRI when assessing hand bone age in forensic age estimation: a pilot study. Forensic Sci Int. 2016;266:281–8.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1(8476):307–10.
Greulich WW, Pyle SI. Radiographic atlas of skeletal development of the hand and wrist. Stanford, California. USA: Stanford University Press; 1959.
Dreizen S, Parker GS, Snodgrasse RM, Spies TD, Webbpeploe H. Bilateral symmetry of skeletal maturation in the human hand and wrist. AMA J Dis Child. 1957;93(2):122–7.
Roche AFA. Study of skeletal maturation in a group of melbourne children. J Paediatr Child Health. 1967;3(3):123–7.
Baer MJ, Djrkatz J. Bilateral asymmetry in skeletal maturation of the hand and wrist: a roentgenographic analysis. Am J Phys Anthropol. 1957;15(2):181–96.
Martin DD, Neuhof J, Jenni OG, Ranke MB, Thodberg HH. Automatic determination of left- and right-hand bone age in the first Zurich longitudinal study. Horm Res Paediatr. 2010;74(1):50–5.
Zheng ZZ, Shan H, Li X. Fat-suppressed 3D T1-weighted gradient-echo imaging of the cartilage with a volumetric interpolated breath-hold examination. AJR Am J Roentgenol. 2010;194(5):W414–9.
Magee T, Shapiro M, Williams D. Comparison of high-field-strength versus low-field-strength MRI of the shoulder. AJR Am J Roentgenol. 2003;181(5):1211–5.
Enders J, Rief M, Zimmermann E, Asbach P, Diederichs G, Wetz C, et al. High-field open versus short-bore magnetic resonance imaging of the spine: a randomized controlled comparison of image quality. PLoS One. 2013;8(12):e83427.
Acknowledgments
Open access funding provided by Medical University of Vienna. We gratefully acknowledge Ms. Ines Fötschl and Mr. Philip Anner, MSc, for graphical processing of the study images.
Funding
The study was part of a research contract between Siemens Healthineers, Siemens Healthcare GmbH, Germany, and Medical University of Vienna, Department of Biological Imaging and Image-guided Therapy (grant no. FA771B0128).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have nothing to disclose.
Ethical approval
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Hojreh, A., Gamper, J., Schmook, M.T. et al. Hand MRI and the Greulich-Pyle atlas in skeletal age estimation in adolescents. Skeletal Radiol 47, 963–971 (2018). https://doi.org/10.1007/s00256-017-2867-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-017-2867-3