
Abstract
Objective
To compare the positions of the trochlear groove (TG) line and the vertical midline of the pericondylar rectangle on axial computed tomography (CT).
Materials and methods
A retrospective pilot study was conducted in February and March 2011 comprising 14 knees in 9 consecutive patients with patellofemoral pain, a normal trochlear angle (124°–145°), and no medical record of prior knee surgery. After the axial CT image displaying the center of the trochlear groove (“reference cut”) with a normal trochlear angle was identified, the pericondylar rectangle was drawn and located in the first quadrant of the Cartesian rectangular coordinate system. The x-coordinates of the vertical lines passing through the most posterior point of the trochlear groove (TG line) and the midpoints of the horizontal sides of the pericondylar rectangle (vertical midline) were obtained at 2-week intervals and statistically analyzed as matched pairs for differences (Wilcoxon signed rank test), agreements (Bland–Altman plot, intraclass correlation coefficient [ICC]) and relative variations (coefficient of variation [CV]).
Results
There were no statistically significant differences between matched pairs (2-tailed p from 0.583 to 0.641) whereas the agreements were substantial (bias = −0.37 and −0.45 respectively, ICC = 0.688 and 0.670 respectively) to almost perfect for duplicate measurements (bias = 0.11 and 0.04 respectively, ICC = 0.975 and 0.998 respectively), with much less relative variation with regard to the vertical midline (CV = 1.22% to CV = 0.34% respectively).
Conclusion
The positions of the TG line and the vertical midline of the pericondylar rectangle on axial CT were identical. The latter was identified regardless of trochlear morphology.
Similar content being viewed by others


Introduction
The extensor mechanism of the knee includes the quadriceps muscle and tendon, the patella, and the patellar ligament [1]. It is believed that increased lateralization of the tibial tuberosity, represented by the tibial tuberosity (TT)–trochlear groove (TG) distance (Fig. 1), is a factor predisposing to patellofemoral instability. The likely outcome is the malalignment of extensor mechanism of the knee [2], and patellofemoral pain, a common musculoskeletal complaint [3].

The TT–TG distance of the right knee. The distance between the tibial tuberosity (TT) and the trochlear groove (TG) defines the alignment of the extensor mechanism of the knee (3D CT image was rendered with InVesalius 3.0. beta 2 software, Renato Archer Information Technology Centre)
To quantify the extent of lateralization, axial computed tomography (CT) is used. Axial CT images showing the center of the tibial tuberosity on the one hand and the center of the trochlear groove on the other are routinely superimposed.
In measuring the TT–TG distance, three lines are drawn [1, 4–7].
The first line passing through the visually approximated positions of the most posterior points of the femoral condyles is called the posterior intercondylar line. The anatomy of the posterior parts of the femoral condyles is usually symmetric and stable [8]. The posterior intercondylar line is therefore a reliable reference line in measuring the TT–TG distance. Some of the close synonyms are: the posterior femoral condylar line [4], the posterior bicondylar line [5], the posterior condylar line [6], and the bicondylar line [7].
The other two lines are vertical to the posterior intercondylar line. The first line passing through the visually approximated position of the most anterior point of the tibial tuberosity is called the TT line [6]. The second line passing through the visually approximated position of the most posterior point of the trochlear groove is called the TG line [6]. The horizontal distance between the TT line and the TG line is called the TT–TG distance [4–7]. A TT–TG distance value greater than 20 mm and patellofemoral pain are perceived as probable indications for knee surgery [7].
The objective of this study was to compare the positions of the TG line and the vertical midline of the pericondylar rectangle on axial CT.
Materials and methods
Materials
A retrospective pilot study was conducted in February and March 2011 at the Clinical Institute of Diagnostic and Interventional Radiology of the Zagreb University Hospital Center in Croatia. Given the retrospective study design, the patients’ written informed consent was not deemed necessary, although the Declaration of Helsinki as revised at the 59th World Medical Association General Assembly in Seoul 2008 was closely followed where applicable.
From the group of consecutive patients that had musculoskeletal CT imaging during the period of this study, 14 knees in 9 patients (7 women, 2 men, mean age 32.22 ± 12.98 years), 4 unilateral and 5 bilateral, were included. Inclusion criteria were as follows: patellofemoral pain, a normal trochlear angle (124°–145°) [7], and no medical record of prior knee surgery.
Methods
The CT positioning protocol was: supine position and quadriceps muscles relaxed with knees in full anatomical extension. The CT imaging protocol was: 43–50 mA, 130 kV, and 2-mm slice thickness at bone window setting (width= 1,500, center = 450). The CT measuring protocol will be described in detail. Below is an introduction to some of the concepts in geometry utilized in the study.
Basic geometry concepts
In Euclidean plane geometry (Euclid, 325–265 BC), a rectangle is a quadrilateral with four vertices at right angles (90°). The horizontal sides of a rectangle are the lower and the upper horizontal side. The vertical sides of a rectangle are the left and the right vertical side. The opposite sides of a rectangle are of the same length. Since they are also parallel, a rectangle is a parallelogram. Moreover, a rectangle has two midlines: the horizontal midline passing through the midpoints of the vertical sides and the vertical midline passing through the midpoints of the horizontal sides.
In Cartesian analytic geometry (Renatus Cartesius alias René Descartes, 1596–1650), the numerically expressed position of a point in a two-dimensional space is called a coordinate. The rectangular coordinate system consists of the horizontal x-axis (the abscissa) and the vertical y-axis (the ordinate) at right angle (90°) to each other, dividing the two-dimensional space into four quadrants (marked by convention with Roman numerals I, II, III, and IV in counter-clockwise order). The intersection of the rectangular coordinate axes is the origin of coordinates (the coordinate 0). A horizontal distance of a point from the origin of coordinates is the x-coordinate. A vertical distance of a point from the origin of coordinates is the y-coordinate. The coordinates make ordered pairs (x, y).
The CT measuring protocol
The CT measuring protocol is schematically summarized in Fig. 2.

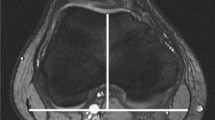
The CT measuring protocol. a The pericondylar rectangle located in the first quadrant of the Cartesian rectangular coordinate system. b The CT measuring protocol of the left knee. RA Roman arch, TG trochlear groove line, TT tibial tuberosity line, TT–TG tibial tuberosity–trochlear groove distance, VM vertical midline of the pericondylar rectangle, asterisk visually approximated position of the most posterior point of the trochlear groove. Orientation box: A anterior, L lateral, M medial, P posterior
Initially, a sequence of axial CT images was obtained. From this a single axial CT image was taken as a reference. The “reference cut” was the axial CT image with a fully recognizable intercondylar groove shaped as a Roman arch, hence displaying the midtrochlear region [5, 7]. It should be noted that the antero-posterior diameter of the Roman arch was approximately one third of the antero-posterior diameter of the femoral condyles [7].
The pericondylar rectangle was drawn with vertices ABCD in counter-clockwise order. The horizontal sides of the pericondylar rectangle ABCD were the lower (AB) and the upper (CD) horizontal side. Notice that the lower horizontal side (AB), passing through the visually approximated positions of the most posterior points of the femoral condyles, was the posterior intercondylar line. The vertical sides of the pericondylar rectangle ABCD were the left (AD) and the right (BC) vertical side.
To ensure that the axial CT image depicts the midtrochlear region, the antero-posterior diameter of the Roman arch was one third of the length of the vertical sides (AD and BC).
Subsequently, the trochlear angle was measured. The value of the trochlear angle between 124° and 145° [7] indicated a normal, groove-shaped midtrochlear region—the center of the trochlear groove—and the respective axial CT image was included in the study.
The pericondylar rectangle ABCD was located in the first quadrant of the Cartesian rectangular coordinate system. Point A was the origin of coordinates.
Depending on the visually approximated position of the most posterior point of the trochlear groove, the position of the TG line varied solely in the horizontal direction (left–right).
In measuring the TT–TG distance, the TG line is always vertical. Therefore, the horizontal distance between any of the points on the TG line and the origin of coordinates was equal. The horizontal distance of a point from the origin of coordinates, as stated previously, is the x-coordinate. Thus, the x-coordinate of the TG line, the length of DE, was measured.
The vertical midline of the pericondylar rectangle was the line passing through the midpoints of the horizontal sides. However, only the length of AB was measured. The x-coordinate of the vertical midline, the length of AF, was calculated as half the length of AB. In addition, the length of AB varied with condylar morphology.
Duplicate measurements of the lengths of DE (DE1 and DE2) and AF (AF1 and AF2), at 2-week intervals, are shown in Table 1.
Statistical analysis
Statistical analysis was performed with MedCalc Software (version 12.0., Mariakerke, Belgium). A p value <0.05 was considered statistically significant. Although the Kolmogorov–Smirnov test could not reject the normality of the data, because of the small sample size [9], the non-parametric Wilcoxon signed rank test for matched pairs was employed to evaluate the difference between medians. Bland–Altman plots [10] were drawn and the single measure of intraclass correlation coefficient (ICC), with a two-way random model and an absolute agreement type, was calculated to analyze the agreement between matched pairs with 95% confidence intervals (CI). Finally, the coefficient of variation (CV) for duplicate measurements was obtained to assess the relative variation.
Results
The results of the statistical analysis are shown in Table 2. There were no statistically significant differences between matched pairs. Also, 95% of differences showed less than 1.96 standard deviation (SD) on the Bland–Altman plots (Fig. 3). According to Landis and Koch [11], substantial agreement was found between the positions of the TG line and the vertical midline of the pericondylar rectangle at 2-week intervals (ICC = 0.688 and 0.670 respectively), with almost perfect agreement of duplicate measurements (ICC = 0.975 and 0.998 respectively). Much less relative variation was observed with regard to the vertical midline (mean = 38.893, SD = 0.475, CV = 1.22% and mean = 39.304, SD = 0.135, CV = 0.34% respectively).

The positions of the TG line (DE1 and DE2) and the vertical midline (AF1 and AF2) of the pericondylar rectangle on axial CT, obtained at 2-week intervals and statistically analyzed as matched pairs for agreement using Bland–Altman plots
Discussion
This retrospective pilot study showed that there was no statistically significant difference between the position of the TG line and the vertical midline of the pericondylar rectangle on axial CT: they were identical.
An interesting point to highlight is that in drawing the vertical midline of the pericondylar rectangle, the trochlear morphology was circumvented.
Trochlear dysplasia is the most frequent condition in patellofemoral instability [12]. Consequently, when the midtrochlear region is not remotely groove-shaped (Fig. 4), the visual approximation of the position of its most posterior point is quite impossible. It can be difficult to decide where to draw the TG line [13, 14]. Since different observers yield different results, this might have a serious bearing on the value of the TT–TG distance. Saudan and Fritschy [15] have suggested that one of the reasons for increased interobserver variability in measuring the TT–TG distance was the labeling of the TG point in the case of major trochlear dysplasia. The corresponding literature seems fairly scarce and few authors have tried to provide a viable solution. Yet, the pericondylar rectangle method implies that drawing the vertical midline instead of the TG line could objectify the measurement of the TT–TG distance in the case of major trochlear dysplasia.

Major trochlear dysplasia of the right knee in three different subjects. The a shallow, b flat or c bumpy midtrochlear region (arrows) makes the visual approximation of its most posterior point on axial CT quite impossible
The main limitation of this retrospective pilot study, apart from the possible selection bias due to design itself, was a small sample size, which made it less able to detect a true difference (type II [β] error). Nevertheless, as this was the first study of its kind, the results could primarily serve as a starting point in estimating the relevant statistical parameters needed for broader studies in the future.
References
Donell S. (IV) Patellofemoral dysfunction—extensor mechanism malalignment. Curr Orthop. 2006;20:103–11.
Dejour D, Vasconcelos W, Tavernier T. Patellofemoral osteoarthritis. In: Bonnin M, Chambat P, eds. Osteoarthritis of the knee. Surgical treatment. Paris: Springer, 2008:24.
Hašpl M, Dubravčić-Šimunjak S, Bojanić I, Pećina M. Anterior knee pain in the sport and work. Arh Hig Rada Toksikol. 2001;52(4):441–9.
Sillanpää P. Radiographs of the patellofemoral joint. In: Traumatic patellar dislocation and clinical significance of medial patellofemoral ligament injury. Academic dissertation. Tampere: Faculty of Medicine of the University of Tampere, 2009:36–7.
Montserrat F. Isolated patellofemoral osteoarthritis. In: Bentley G. ed. European instructional lectures. 11th EFORT Congress, Madrid, Spain. Dordrecht: Springer, 2010:169–70.
Manaster BJ. Section IV. Angles and measurements. Knee/leg, angles and measurements. Lateral translation: TT–TG method. In: Manaster BJ, Crim J, Rosenberg ZS. Diagnostic and surgical imaging anatomy. Knee, ankle, foot. Salt Lake City: Amirsys; 2007:5.
Beaconsfield T, Pintore E, Maffulli N, Petri GJ. Radiological measurements in patellofemoral disorders. A review. Clin Orthop Relat Res. 1994;308:18–28.
Fulkerson JP. Imaging the patellofemoral joint. Performing patellofemoral CT. In: Disorders of the patellofemoral joint. 4th ed. Philadelphia: Lippincott Williams & Wilkins, 2004:89.
Dawson B, Trapp RG. Basic and clinical biostatistics. 4th ed. New York: Lange Medical Books/McGraw-Hill; 1994. p. 138–9.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307–10.
Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159–74.
Burmann RC, Locks R, Pozzi JFA, Konkewicz ER, de Souza MP. Evaluation of predisposing factors in patellofemoral instabilities. Acta Ortop Bras. 2011;19(1):37–40.
Pietsch M, Hofmann S. Value of radiographic examination of the knee joint for the orthopedic surgeon. Radiologe. 2006;46(1):55–64.
Julliard R, Ligeon R. Major dysplasia of the trochlea. Contribution to the measurement of the A.T. T.G. value. Proposal for a CT examination procedure. J Radiol. 1992;73(6–7):403–7.
Saudan M, Fritschy D. AT-TG (anterior tuberosity-trochlear groove): interobserver variability in CT measurements in subjects with patellar instability. Rev Chir Orthop Reparatrice Appar Mot. 2000;86(3):250–5.
Acknowledgments
The author is very grateful to Prof. Kristina Potočki, M.D., Ph.D., for her general support, Neva Coce, M.D., for her intellectual input and invaluable suggestions, Mrs. Sofija Herceg at the Zagreb University Hospital Center Medical Library for her assistance in gathering the articles used in this paper and Mr. Mohammad Imran Khan Malik, BSc, for editing the English version of the manuscript.
Funding
None.
Conflict of interest
The author declares no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nizić, D. Comparison of positions of the trochlear groove line and the vertical midline of the pericondylar rectangle on axial computed tomography: a retrospective pilot study. Skeletal Radiol 41, 1099–1104 (2012). https://doi.org/10.1007/s00256-011-1346-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-011-1346-5