
Abstract
Isolated noncompaction of the ventricular myocardium is a cardiomyopathy influencing almost exclusively the left ventricle in children and adults. We report a case of a neonate presenting with right ventricular failure caused by a noncompaction of the right ventricle. However, later course of the disease demonstrated biventricular involvement. Right ventricular noncompaction can be a cause of early postnatal right ventricular failure.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Isolated noncompaction of the left ventricular myocardium is a rare but often reported form of cardiomyopathy in children [7] and adults [10] in which the embryonic pattern of myoarchitecture focally persists along with a lacunary blood supply [5]. However, right ventricular involvement is extremely rare [2]. We report a case in which noncompaction affected initially the right ventricular myocardium only and led to heart failure soon after birth.
Case Report
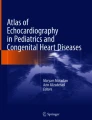
A full-term 2-day-old female neonate, a product of uncomplicated pregnancy of consanguine Turkish parents (birth weight, 3300 g), was admitted to the neonatal intensive care unit after she experienced a circulatory collapse. Her peripheral pulsations were diminished, with features of poor peripheral circulation and anuria. Coarse facial features and a broad nasal bridge were present. The liver was palpable 2 cm below the costal margin. The cardiac auscultatory findings were normal. Electrocardiography (ECG) showed abnormal tall P waves in II and V1, abnormal low voltage in V1, and flat T waves in V5–V6, along with sporadic premature ventricular contractions of right ventricular origin. Echocardiography demonstrated a structurally normal heart. The right ventricle (RV) and right atrium were dilated. All three components of the RV were developed, but the apical area appeared grossly abnormal, with the trabecular meshwork with deep intertrabecular recesses occupying the whole of the RV apex (Fig. 1). The RV exhibited both systolic and diastolic dysfunction, with the latter being predominant. The interatrial septum bulged markedly from right to left during diastole, returning to the midline in systole. Pulmonary hypertension was not present. The left ventricular (LV) apex seemed unaffected, and the LV function was normal. Artificial ventilation, inotropic support, and diuretics were started. The infant was weaned off the ventilator 6 days later. Premature ventricular contractions disappeared. Although the patient remained clinically stable, repeated echocardiography demonstrated mild LV systolic dysfunction (SF 0.23) and mitral regurgitation grade 2 on the tenth postnatal day. Contrary to earlier studies, the development of minimal involvement of the LV apex consistent with an additional noncompaction of the myocardium of the LV has been noted. Studies performed to elicit an infectious or genetic cause of the myocardial failure were negative. Oral digoxin and diuretic treatment was maintained and subsequently stopped; the LV size and function gradually improved to completely normal and mitral regurgitation disappeared. However, after 8 months of favorable findings, the isolated left ventricular dysfunction along with mitral insufficiency reappeared. Despite treatment with captopril and digoxin, the LV function deteriorated, necessitating short-term intravenous inotropic support.

Two-dimensional apical four-chamber view demonstrated trabecular meshwork with deep intertrabecular recesses occupying the whole of the right ventricular apex (arrows). LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.
The patient has been followed for 4 years. She has remained clinically well without any regular medication. There have been no clinical features of right or left-sided heart failure. However, echocardiography has remained grossly abnormal. The noncompaction has seemed to be biventricular, although the spongy myocardium of the apical portion of the LV has occupied much less space than the analogical structures within the RV. The systolic and diastolic dysfunction of the right heart has still dominated. Whereas the cross-sectional area of the left atrium was normal (108% of normal values), the right atrial area was increased up to 216% of normal values. The ratio of right/left atrial area was 1.88. Pulsed Doppler revealed features of impaired right ventricular relaxation, and there was an abnormal motion pattern of the interventricular septum. Left ventricular end systolic diameter was increased (141% of normal values), leading to a decreased shortening fraction of the LV of 0.20. Mild tricuspid and mitral regurgitation was demonstrated.
Discussion
Isolated noncompaction of the ventricular myocardium is being reported with increasing frequency as a cause of ventricular failure in adults and children. It has been described in association with congenital heart defects, most often outflow obstructive lesions or coronary anomalies, but in its isolated form it represents a specific cardiomyopathy. It is believed to result from a persistence of an early embryonic stage [5], sharing morphological similarities with the spongy myocardium of fish, amphibians, and reptiles. Illustrative echocardiographic appearance of such a spongy myocardium of a crocodile has been published [6]. In a series of 34 adult patients, noncompaction affected exclusively the LV [10]. However, it is not the spongy appearance of the myocardium alone that is necessary for the diagnosis of the noncompaction. Echocardiographic features of noncompaction most often described include multiple ventricular trabeculations; color Doppler evidence of multiple, deep intratrabecular recesses communicating with the ventricular cavity; and ventricular dilatation with reduced systolic and/or diastolic ventricular function. In fact, prominent left ventricular trabeculations can be found in many hypertrophic hearts, and thus our threshold to diagnose noncompaction may be artificially low. Clear-cut echocardiographic diagnostic criteria are therefore warranted. Quantification with the echocardiographic X-to-Y ratio has been used [3], comparing distance between epicardial surface and trough of a trabecular recess (X) and the distance between the epicardial surface and peak of the trabeculation (Y). A ratio of thicker noncompacted myocardium on the endocardial side and a thin compacted myocardium on the epicardial side ≥2 was reported to be diagnostic [10]. In the future, tissue Doppler echocardiography may provide the features pathognomonic for noncompaction [12].
The right ventricular apex with hypertrophic trabeculae separated by fissures can be even more challenging. The right ventricular involvement is assessed on a purely qualitative basis [11]. In contrast with postnatal experience, in the fetus, the disease is seen mostly in the RV [8].
Although involvement of the fetal LV was echocardiographically not evident in some cases, histological data showed that the LV is not spared by the disease during fetal life [9]. This must have been the case for our patient. Although the left ventricular involvement was not convincing after birth, the noncompaction on the left side became evident later. Postnatal minimal involvement of the left ventricular apex did not meet quantitative criteria for noncompaction. Lack of obvious left ventricular abnormality, compared to the right side, explains why noncompaction of the LV was only identified at a later stage. If noncompaction as a result of earlier spongy fetal myocardium, it must have been present postnatally.
In some patients, familial occurrence of this disorder can occur, suggesting a genetical substrate. Xq28-linked noncompaction of the left ventricular myocardium may share some phenotypic overlap with the Barth syndrome [1], but reports on affected female patients including our case indicate a genetic heterogeneity of the process [4].
In conclusion, although the cardiomyopathy caused by noncompaction of the ventricular myocardium in children and adults affects almost exclusively the LV in neonates the noncompaction can cause right heart failure.
References
SB Bleyl BR Mumford MC Brown-Harrison et al. (1979) ArticleTitleXq28-linked noncompaction of the left ventricular myocardium: prenatal diagnosis and pathologic analysis of affected individuals Am J Med Genet 72 257–265
Y Cavusoglu N Ata B Timuralp et al. (2003) ArticleTitleNoncompaction of the ventricular myocardium: report of two cases with bicuspid aortic valve demonstrating poor prognosis and with prominent right ventricular involvement Echocardiography 20 379–383 Occurrence Handle12848883 Occurrence Handle10.1046/j.1540-8175.2003.03045.x
TK Chin JK Perloff RG Williams K Jue R Mohrmann (1990) ArticleTitleIsolated noncompaction of left ventricular myocardium. A study of eight cases Circulation 82 507–513 Occurrence Handle2372897 Occurrence Handle1:STN:280:DyaK3czit1GksQ%3D%3D
MC Digilio B Marino M Bevilacqua et al. (1999) ArticleTitleGenetic heterogeneity of isolated noncompaction of the left ventricular myocardium Am J Med Genet 85 90–91 Occurrence Handle10377021 Occurrence Handle1:STN:280:DyaK1MzgtlGitg%3D%3D
J Dusek B Ostadal M Duskova (1975) ArticleTitlePostnatal persistence of spongy myocardium with embryonic blood supply Arch Pathol 99 312–317 Occurrence Handle1147832 Occurrence Handle1:STN:280:DyaE2M3gsVGqtQ%3D%3D
FJ Halbertsma LGFM van't Hek O Daniels (2001) ArticleTitleSpongy cardiomyopathy in a neonate Cardiol Young 11 458–460 Occurrence Handle11558958 Occurrence Handle1:STN:280:DC%2BD3MrhtVymsw%3D%3D
F Ichida Y Hamamichi T Miyawaki et al. (1999) ArticleTitleClinical features of isolated noncompaction of the ventricular myocardium J Am Coll Cardiol 34 233–240 Occurrence Handle10400016 Occurrence Handle10.1016/S0735-1097(99)00170-9 Occurrence Handle1:STN:280:DyaK1MzisFKjsQ%3D%3D
AA Karatza SE Holder HM Gardiner (2003) ArticleTitleIsolated noncompaction of the ventricular myocardium: prenatal diagnosis and natural history Ultrasound Obstet Gynecol 21 75–80 Occurrence Handle12528168 Occurrence Handle10.1002/uog.10 Occurrence Handle1:STN:280:DC%2BD3s%2FitFCgsA%3D%3D
C Moura Y Hillion F Daikha-Dahmane et al. (2002) ArticleTitleIsolated non-compaction of the myocardium diagnosed in the fetus: two sporadic and two familial cases Cardiol Young 12 278–283 Occurrence Handle12365176
EN Oechslin CH Attenhofer Jost JR Rojas PA Kaufmann R Jenni (2000) ArticleTitleLong-term follow-up of 34 adults with isolated left ventricular noncompaction: a distinct cardiomyopathy with poor prognosis J Am Coll Cardiol 36 493–500 Occurrence Handle10933363 Occurrence Handle10.1016/S0735-1097(00)00755-5 Occurrence Handle1:STN:280:DC%2BD3czpslSgtA%3D%3D
M Ritter E Oechslin G Sutsch et al. (1997) ArticleTitleIsolated noncompaction of the myocardium in adults Mayo Clinic Proc 72 26–31 Occurrence Handle1:STN:280:DyaK2s7kvVKltA%3D%3D Occurrence Handle10.4065/72.1.26
RI Williams ND Masani MB Buchalter AG Fraser (2003) ArticleTitleAbnormal myocardial strain rate in noncompaction of the left ventricle J Am Soc Echocardiogr 16 293–296 Occurrence Handle12618740
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hruda, J., Sobotka-Plojhar, M. & Fetter, W. Transient Postnatal Heart Failure Caused by Noncompaction of the Right Ventricular Myocardium. Pediatr Cardiol 26, 452–454 (2005). https://doi.org/10.1007/s00246-004-0752-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-004-0752-z