
Abstract
Purpose
To investigate the prevalence and initiation of statins as well as treatment intensity in the oldest old, with younger olds as a reference.
Methods
A population-based cohort was used, including record-linked data from the Total Population Register, the Swedish Prescribed Drug Register, and the Swedish Patient Register. In each year over the study period (2009–2015), statin use was described in individuals 85 years or older and 65–84 years of age, and initiation rates were calculated among individuals with no statin treatment during a preceding 3-year period.
Results
A total of 1,764,836 individuals ≥ 65 years in 2009, increasing to 2,022,764 in 2015, were included in the analyses. In individuals 85 years or older, the prevalence of statin therapy increased from 11% in 2009 to 16% in 2015, the corresponding initiation rates being 1.3% and 1.7%, respectively. Corresponding prevalence and incidence figures in 65–84-year-olds were 23 to 25% and 3.0 to 3.3%, respectively. Overall, the proportion of individuals initiating statin with high-intensity treatment (atorvastatin ≥ 40 mg or rosuvastatin ≥ 20 mg) in the oldest old increased from 1 to 36% during the study period, and a similar increase was seen in the younger age group. Over the study years, the presence of an established indication for statin treatment varied between 70 and 76% in the oldest old and between 30 and 39% in the younger olds.
Conclusion
Prevalence and initiation of statin therapy are increasing among the oldest old, despite the fact that randomized controlled trials focusing on this age group are lacking and safety signals are difficult to detect.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Statin treatment is important in cardiovascular disease and has been proven effective in reducing major vascular events and mortality, especially in secondary prevention [1,2,3,4,5,6,7]. However, the large randomized controlled studies with statins have not included a significant proportion of older individuals. For example, the pivotal 4S study only included individuals 35–70 years of age [7], and the primary prevention WOSCOPS study included only males aged 45–64 years [6]. The latest meta-analysis by the Cholesterol Treatment Trialists (CTT) collaboration, focusing on advancing age on major endpoints in 28 statin trials, showed that the relative risk reduction was less in participants over 75 years of age and not statistically significant among those without the previous vascular disease [8]. There are limitations also in this meta-analysis—among others a low proportion of older patients (8% were 75 years or older) and that the included trial populations were selected with fewer comorbidities than normally seen at older ages. Another recent meta-analysis, however, suggests beneficial effects in those 75 years or older [9]. Nevertheless, the relatively high use of statins among the oldest old could be questioned due to the short life expectancy and sparsity of evidence for an effect in this age group.
In a previous population-based study on statin use in older people according to age and indication [10], we found a relatively high prevalence of statin users. That is, 17% of all individuals ≥ 80 years of age were on statins in 2010, compared with 23% in the age group 65–80 years. Therefore, as randomized controlled trials of the benefit-risk balance for statin therapy in this age group are sparse, we further studied the use of statins in the oldest old, by investigating the prevalence and initiation of statins, as well as treatment intensity, in those 85 years or older, with younger olds as a reference. We also explored the use according to initiating specialty, with a focus on statin type, treatment intensity, and treatment duration.
Method
Study population
The study population included all individuals 65 years or older, who lived in Sweden during the period January 1, 2009, to December 31, 2015, or part of this period.
For each year, the study population was defined as follows: Individuals were included in the yearly population from the year they turned 65. For example, an individual born in 1945 was included in the population from 2010 onwards. Individuals who died during the study period were excluded from the population from the year after they died. Thus, an individual who died in 2012 was included in the 2012 population, but not from 2013 and onwards. Individuals who immigrated were included in the population from the year after immigration and individuals who emigrated were excluded from the population from the year of emigration. A total of 107 individuals with incomplete or ambiguous immigration/emigration dates, or re-used personal identity numbers, were excluded from the study.
Data sources
Data were collected from three population-based registers, linked by the unique personal identity number:
-
The Total Population Register at Statistics Sweden provided information about who were residents in Sweden, as well as dates of deaths and moving into/out of the country during the study period [11, 12].
-
The Swedish Prescribed Drug Register (SPDR) at the Swedish National Board of Health and Welfare provided information on all prescribed drugs dispensed in any pharmacy in Sweden [13].
-
The Swedish Patient Register [14] contains data from all inpatient stays and specialized outpatient visits in Sweden. The diagnoses are registered according to the International Statistical Classification of Diseases and Related Health Problems (ICD-10).
Definitions and procedures
The prevalence of statin use was calculated each year from 2009 to 2015. An individual was classified as a prevalent statin user each year if he/she filled statin prescriptions (codes C10AA or C10BA in the Anatomical Therapeutic Chemical classification system (ATC) [15] covering at least 75% of the year. Swedish regulations stipulate drugs can be dispensed for a maximum of 3-month use at a time. Thus, our definition of a statin user was ≥ 3 filled statin prescriptions over a year. Individuals who had at least one drug dispensed within the multi-dose drug-dispensing (MDD) system and therefore had drugs delivered every fortnight were classified as statin users if they had ≥ 20 statin dispensations over the year.
For each year from 2009 to 2015, we also calculated the proportions of the different statin types used among the statin users. A specific statin (simvastatin, fluvastatin, pravastatin, atorvastatin, cerivastatin, rosuvastatin, or pitavastatin; ATC codes C10AA01, C10AA03-C10AA05, C10AA07, C10AA08) or combination drugs (simvastatin/ezetimibe, pravastatin/fenofibrate, simvastatin/fenofibrate, atorvastatin/ezetimibe, or rosuvastatin/ezetimibe; ATC codes C10BA02-C10BA06) was classified as used by each individual and year if he/she had at least one filled prescription, or one multi-dose dispensation, of the specific statin that year. The proportion of each statin was then calculated by dividing the number of individuals using the statin by the total number of statin users.
For each year, 2009 to 2015, a person was defined as a statin initiator that year if he/she filled a statin prescription (ATC codes C10AA or C10BA) for the first time during this year, not having used a statin in the previous 3 years. A few individuals, who initiated treatment a second time, within the study period, after a washout period of 3 years, were defined as statin initiators twice.
For each filled prescription, a start date and an end date were defined. The start date was defined as the date of fill. The end date was calculated by estimating the number of days the prescription would last and adding it to the date of fill. The number of days a prescription would last was calculated by dividing the amount of drug dispensed by the prescribed dosage, for ordinary prescriptions, and set to 14 days for drugs delivered within the MDD system. The procedure has been described previously [16].
Treatment duration was defined as the difference between the first date of the first filled prescription and the calculated end date of the last filled prescription. A gap of 6 months between the end date of one prescription and the first date of the next was allowed. When there was a gap of more than 6 months, the last day of treatment was defined as the end date of the last filled prescription before this gap. Sensitivity analyses were performed with an alternative that allowed a gap of 3 months. For those deceased during treatment, the death date was considered the end date of treatment. When calculating treatment duration, only individuals still alive during the follow-up period were included.
Statin daily dose intensity was defined according to guidelines by the American College of Cardiology/American Heart Association (ACC/AHA) [17], as low intensity: fluvastatin < 80 mg, pitavastatin < 2 mg, pravastatin < 40 mg, or simvastatin < 20 mg; moderate intensity: atorvastatin ≥ 10 < 40 mg, fluvastatin ≥ 80 mg, pitavastatin ≥ 2 mg, pravastatin ≥ 40 mg, rosuvastatin ≥ 10 < 20 mg, or simvastatin ≥ 20 mg; and high intensity: atorvastatin ≥ 40 mg or rosuvastatin ≥ 2 0 mg. The prescribed daily dose (PDD) was calculated by dividing the prescribed daily dose by the defined daily dose (DDD) according to the World Health Organization (WHO) [15], which was for rosuvastatin 10 mg, atorvastatin 20 mg, simvastatin, and pravastatin 30 mg, and fluvastatin 60 mg.
Information regarding the setting of the initiating prescriber was retrieved from the SPDR and merged into five categories: general practice, internal medicine (also including cardiology and neurology since these specialties are included in the department of internal medicine in many smaller hospitals in Sweden), surgery, geriatrics, and other, which included the remaining specialties.
ICD-10 diagnoses from inpatient and specialized outpatient care, recorded over the 5-year period preceding statin initiation, were retrieved from the Swedish Patient register. The following established indications were extracted, being considered relevant for statin treatment: ischemic heart disease (ICD-10 I20-I25), cerebrovascular disease (ICD-10 I63-I67, I69.3), TIA (ICD-10 G45), cerebral vascular syndromes (ICD-10 G46), atherosclerosis (ICD-10 I70), and diabetes (ICD-10 E10-14).
Descriptive analyses were performed using STATA (Version 14) and SPSS (IBM SPSS Statistics for Windows, version 23.0, Armonk, NY).
Results
Study population
The population of Swedish inhabitants, 85 years or older, consisted of 288,737 individuals in 2009 and 301,065 individuals in 2015 (Fig. 1, Table 1). The proportion of women was 66% in 2009 and 65% in 2015 and the mean age was 88.9 in 2009 and 89.3 in 2015. The population of younger olds, 65–84 years, was 1,476,099 individuals in 2009 and 1,721,699 in 2015 (Appendix 1).

Flowchart of the study population 2009–2015
Statin prevalence
Among the oldest old (≥ 85 years), 11% were statin users in 2009 and 16% in 2015. The use of simvastatin decreased from 87% in 2009 to 74% in 2015 (p < 0.001) while atorvastatin increased from 8% in 2009 to 22% in 2015 (p < 0.001). Pravastatin and rosuvastatin were used to a smaller extent, as well as fluvastatin and the combination simvastatin/ezetimibe (Table 2). Among the younger old (65–84 years), 23% were statin users in 2009 and 25% in 2015 (Appendix 2).
Statin initiators
In the oldest age group (≥ 85 years), statin initiation increased during the study period, from 1.3 to 1.7% (p < 0.001) (Table 2). In 2009, simvastatin was the most frequently initiated statin, with 98% receiving this drug, compared with 31% in 2015. During the study period, atorvastatin became more common and was in 2014 and 2015 the most frequently initiated statin, with 57% of the new prescriptions in 2014 and 68% in 2015 (Table 2). Throughout the study period, initiation of a statin was more frequent in the younger age group (65–84 years), 3.0% in 2009 and 3.3% in 2015 (p < 0.001) (Appendix 2).
During the study period, a shift towards more intensive treatment was seen in the oldest old. In 2009, 1% was being prescribed high-intensity treatment, whereas the corresponding figure in 2015 was 36% (p < 0.001) (Table 2). A similar shift towards high-intensity treatment was seen in the younger olds. The mean PDD at statin initiation was higher for atorvastatin and varied more during the study period, compared with simvastatin.
For statin initiators in the oldest age group, the proportion who discontinued treatment within the first 100 days was 21 to 24% in 2009–2014 (Table 2). In all, 32% in 2009, and 40% in 2013, continued their statin treatment for more than 2 years. An established indication was found for 70% in 2009 and for 75% in 2015. The corresponding figures for the younger olds were 29% and 39%, respectively (Appendix 2).
Statin prescribing by prescriber setting
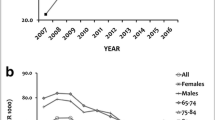
During the entire study period, statins in the oldest old (≥ 85 years) were most often initiated from internal medicine, 46% in 2009 and 53% in 2015; the second most frequent initiating setting being primary care, 27% in 2009 and 23% in 2015 (Table 3). Over the study period, PDD and treatment intensity were higher in those who had their statin treatment initiated from internal medicine compared with primary care, and the proportion of high-intensity treatment increased during the study period (Fig. 2). In younger olds (65–84 years), statins were most often initiated from primary care, 49% in 2009 and 52% in 2015 (Appendix 3).

Proportion of high-intensity treatment, i.e., either atorvastatin ≥ 40 mg or rosuvastatin ≥ 20 mg, initiated over the study years (2009–2915), by the setting of the initiating prescriber
Discussion
In this nationwide population-based study, we found that the overall prevalence of statin users in the oldest old increased from 11% in 2009 to 16% in 2015. In this age group, more individuals initiated statin treatment at the end of the study period, and a shift towards high-intensity treatment was seen. In comparison, statin use was more common in younger olds over the entire study period but did not increase as conspicuously. A similar shift towards high-intensity statin treatment was, however, noted.
The overall increase in statin prevalence in older people is similar to that reported in other studies [18]. However, our finding that statin use increased markedly also in the oldest old deserves attention. Although a recent systematic review and meta-analysis suggest beneficial effects in those 75 years or older [9], the benefit-risk balance in the oldest old in general, including frail individuals with short life expectancy, is still uncertain. Perhaps an ongoing RCT, including 18,000 patients 70 years or older and studying atorvastatin 40 mg, may add further insights (NCT02099123); the size of that study may perhaps allow subgroup analyses of the oldest old and those who develop frailty over the study period. Nevertheless, it must be acknowledged that studying benefits and risks in the oldest old imply challenges; heterogeneity and gradually declining health may aggravate the potential to detect efficacy and safety aspects of preventive treatment.
An increase in statin prevalence among the oldest old could be explained by an expanded prescribing of statins at younger ages, continuing over the years, or by an increased initiation of treatment at older ages. Our results suggest that both alternatives may have contributed to the increased statin prevalence in this age group. Indeed, clinicians may find it difficult to withdraw statin treatment as patients age; there is no clearcut point at the individual level where such treatment does not add any benefit. Furthermore, our results show an increased initiation of statin treatment over the years.
In the study population as a whole, nearly every other statin initiator in 2015 received their first prescription from primary care. This finding is consistent with a previous study [19]. In the oldest olds, however, more than every second statin initiator instead had their first prescription from an internal medicine setting. Geriatricians, on the other hand, initiate statin treatment only to a small extent, a finding that may be explained by the fact that they treat the oldest and most frail patients with a short life expectancy and therefore uncertainties regarding beneficial effects. Furthermore, almost nine in ten of these patients had an underlying established indication for statin treatment. These results are in line with our previous study, where old age was positively associated with the presence of an established indication, suggesting that this age group is more often prescribed statins for secondary prevention [10].
During the study period, a shift towards higher intensity treatment was seen in statin initiators. In 2015, as much as 36% of oldest olds were prescribed high-intensity treatment, compared with only 1% in the oldest age group in 2009. The same shift was seen in the younger age group. This change can be explained by the fact that simvastatin was replaced by atorvastatin as the most prescribed statin during these years, which, in turn, may be due to the fact that the patent for atorvastatin expired in 2012, resulting in a marked price reduction making simvastatin and atorvastatin similarly priced. Another explanation could be a trend towards choosing higher intensity treatment with statins, especially in the hospital setting. ACC/AHA guidelines recommend high-intensity statin treatment for secondary prevention in men and women < 75 years of age and a large observational study found a small but significant survival advantage associated with high intensity, compared with moderate-intensity, statins [20]. We found that, in 2015, eight in ten individuals in the oldest old group received atorvastatin when initiated from internal medicine, whereas simvastatin and atorvastatin were about equally prescribed upon statin initiation in primary care. We have not found many similar studies analyzing the dose of atorvastatin compared with simvastatin, but one earlier study reported that PDD, in relation to DDD, was in general higher for atorvastatin [21].
Strengths and limitations
An important strength of this study is that it comprises the entire older population in Sweden. Additionally, it covers a long period of time, from 2006 to 2015, which allows examination of longer time trends in the initiation of drug therapy. Another strength is that the wealth of information in the SPDR makes it possible to study not only drug use but also doses. Limitations include that the SPDR only records prescription drugs dispensed at pharmacies. Drugs administered in hospitals or from drug storerooms in nursing homes are not recorded in the register, potentially leading to an underestimation of the actual drug exposure. Furthermore, a general limitation of studies based on drug register data is that dispensed drugs may not reflect what is actually taken by the patient. On the other hand, repeated drug fills indicate that the patient is actually using the drug over time. Another limitation is that the information on diagnoses in the present study was based only on data recorded from inpatient and specialized outpatient care. However, the vast majority of established indications consist of conditions that require hospital care, and therefore, this limitation may have had less effects on the results. Furthermore, it may be regarded as a limitation that we did not differentiate our results between secondary prevention (ischemic heart disease and/or cerebrovascular disease) and primary prevention. Indeed, statin treatment for secondary prevention is reportedly less common in those 80 years or older compared with younger olds [10].
Conclusion
This register-based study shows that statin prevalence and incidence, as well as treatment intensity and duration in statin initiators, is increasing in the oldest old. As many older people are exposed to statins—drugs that may also imply a risk of adverse reactions—and also quite often at high doses, further studies evaluating the benefit-risk balance, including the potential quality-of-life gain/loss, are needed to guide clinicians in the process of prescribing.
Availability of data and material
Dr Fastbom and Mrs Sundvall had full access to all data and take responsibility for the integrity of the data and accuracy of the data analysis.
Code availability
Dr Fastbom has full access to the data registry (non-identifiable person data). Acquisition, analysis, and analysis of data: Sundvall, Fastbom.
References
Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, Goldberg AC, Gordon D, Levy D, Lloyd-Jones DM, McBride P, Schwartz JS, Shero ST, Smith SC, Jr., Watson K, Wilson PW (2014) 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 63 (25 Pt B):2889–2934. https://doi.org/10.1016/j.jacc.2013.11.002
Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL et al (2016) 2016 European Guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Atherosclerosis 252:207–274. https://doi.org/10.1016/j.atherosclerosis.2016.05.037
Serruys PW, de Feyter P, Macaya C, Kokott N, Puel J, Vrolix M, Branzi A, Bertolami MC, Jackson G, Strauss B, Meier B (2002) Fluvastatin for prevention of cardiac events following successful first percutaneous coronary intervention: a randomized controlled trial. JAMA 287(24):3215–3222
Heart Protection Study Collaborative Group (2002) MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet 360(9326):7–22. https://doi.org/10.1016/s0140-6736(02)09327-3
The long term intervention with pravastatin in ischaemic disease (lipi) study group (1998) Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med 339 (19):1349-1357. https://doi.org/10.1056/nejm199811053391902
Shepherd J, Cobbe SM, Ford I, Isles CG, Lorimer AR, MacFarlane PW, McKillop JH, Packard CJ (1995) Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. West of Scotland Coronary Prevention Study Group. N Engl J Med 333(20):1301–1307. https://doi.org/10.1056/nejm199511163332001
Scandinavian Simvastatin Survival Study Group (1994) Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 344(8934):1383–1389
Collaboration CTT (2019) Efficacy and safety of statin therapy in older people: a meta-analysis of individual participant data from 28 randomised controlled trials. Lancet 393(10170):407–415. https://doi.org/10.1016/s0140-6736(18)31942-1
Gencer B, Marston NA, Im K, Cannon CP, Sever P, Keech A, Braunwald E, Giugliano RP, Sabatine MS (2020) Efficacy and safety of lowering LDL cholesterol in older patients: a systematic review and meta-analysis of randomised controlled trials. Lancet 396(10263):1637–1643. https://doi.org/10.1016/s0140-6736(20)32332-1
Sundvall H, Fastbom J, Wallerstedt SM, Vitols S (2019) Use of statins in the elderly according to age and indication-a cross-sectional population-based register study. Eur J Clin Pharmacol 75(7):959–967. https://doi.org/10.1007/s00228-019-02645-w
Ludvigsson JF, Almqvist C, Bonamy AK, Ljung R, Michaelsson K, Neovius M et al (2016) Registers of the Swedish total population and their use in medical research. Eur J Epidemiol 31(2):125–136. https://doi.org/10.1007/s10654-016-0117-y
Ludvigsson JF, Otterblad-Olausson P, Pettersson BU, Ekbom A (2009) The Swedish personal identity number: possibilities and pitfalls in healthcare and medical research. Eur J Epidemiol 24(11):659–667. https://doi.org/10.1007/s10654-009-9350-y
Wettermark B, Hammar N, Fored CM, Leimanis A, Otterblad Olausson P, Bergman U et al (2007) The new Swedish Prescribed Drug Register–opportunities for pharmacoepidemiological research and experience from the first six months. Pharmacoepidemiol Drug Saf 16(7):726–735. https://doi.org/10.1002/pds.1294
Ludvigsson JF, Andersson E, Ekbom A, Feychting M, Kim JL, Reuterwall C et al (2011) External review and validation of the Swedish national inpatient register. BMC Public Health 11:450. https://doi.org/10.1186/1471-2458-11-450
ACC/AHA (2013) Guidelines for ATC classification and DDD assignment 2013. In: ed. WHO Collaborating Centre for Drug Statistic Methodology
Wallerstedt SM, Fastbom J, Johnell K, Sjöberg C, Landahl S, Sundström A (2013) Drug treatment in older people before and after the transition to a multi-dose drug dispensing system–a longitudinal analysis. PLoS ONE 8(6):e67088. https://doi.org/10.1371/journal.pone.0067088
Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, Goldberg AC, Gordon D, Levy D, Lloyd-Jones DM, McBride P (2014) 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2889–2934. https://doi.org/10.1016/j.jacc.2013.11.002
Bertolotti M, Franchi C, Rocchi MB, Miceli A, Libbra MV, Nobili A et al (2017) Prevalence and Determinants of the Use of Lipid-Lowering Agents in a Population of Older Hospitalized Patients: the Findings from the REPOSI (REgistro POliterapie Societa Italiana di Medicina Interna) Study. Drugs Aging 34(4):311–319. https://doi.org/10.1007/s40266-017-0448-8
Ofori-Asenso R, Ilomäki J, Tacey M, Zomer E, Curtis AJ, Bell JS et al (2018) Patterns of statin use and long-term adherence and persistence among older adults with diabetes. J Diabetes 10(9):699–707. https://doi.org/10.1111/1753-0407.12769
Rodriguez F, Maron DJ, Knowles JW, Virani SS, Lin S, Heidenreich PA (2017) Association Between Intensity of Statin Therapy and Mortality in Patients With Atherosclerotic Cardiovascular Disease. JAMA cardiology 2(1):47–54. https://doi.org/10.1001/jamacardio.2016.4052
Hartz I, Sakshaug S, Furu K, Engeland A, Eggen AE, Njølstad I, Skurtveit S (2007) Aspects of statin prescribing in Norwegian counties with high, average and low statin consumption - an individual-level prescription database study. BMC Clin Pharmacol 7:14. https://doi.org/10.1186/1472-6904-7-14
Funding
Open access funding provided by Karolinska Institute. The study was supported by the Swedish Research Council for Health, Working Life and Welfare (Forte) (grant no: 2017–01764) and Karolinska Institutet. The funding sources did not influence the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.
Author information
Authors and Affiliations
Contributions
Study concept and design: all authors. Drafting of manuscript: all authors. Critical revision of the manuscript: all authors.
Corresponding author
Ethics declarations
Ethical approval
Regional Ethical Review Board in Stockholm (dnr 2013/1941–31/3 and 2015/1319–32).
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sundvall, H., Vitols, S., Wallerstedt, S.M. et al. Prevalence and initiation of statin therapy in the oldest old—a longitudinal population-based study. Eur J Clin Pharmacol 78, 1459–1467 (2022). https://doi.org/10.1007/s00228-022-03343-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-022-03343-w