
Abstract
Summary
We have produced paediatric reference data for forearm sites using the Stratec XCT-2000 peripheral quantitative computed tomography scanner. These data are intended for clinical and research use and will assist in the interpretation of bone mineral density and bone geometric parameters at the distal and mid-shaft radius in children and young adults aged between 6–19 years.
Introduction
Peripheral quantitative computed tomography (pQCT) provides measurements of bone mineral content (BMC), density (BMD) and bone geometry. There is a lack of reference data available for the interpretation of pQCT measurements in children and young adults. The aim of this study was to provide reference data at the distal and mid-shaft radius.
Methods
pQCT was used to measure the 4% and 50% sites of the non-dominant radius in a cohort of healthy white Caucasian children and young adults aged between 5 and 25 years. The lambda, mu, sigma (LMS) technique was used to produce gender-specific reference centile curves and LMS tables for calculating individual standard deviations scores.
Results
The study population consisted of 629 participants (380 males). Reference centile curves were produced; total and trabecular BMD for age (distal radius) and for age and height, bone area (distal and mid-shaft radius), cortical area, cortical thickness, BMC, axial moment of inertia, stress–strain index and muscle area (mid-shaft radius).
Conclusions
We present gender-specific databases for the assessment of the distal and mid-shaft radius by pQCT. These data can be used as control data for research studies and allow the clinical interpretation of pQCT measurements in children and young adults by age and height.



Similar content being viewed by others


References
Binkley TL, Specker BL, Wittig TA (2002) Centile curves for bone densitometry measurements in healthy males and females ages 5–22 yr. J Clin Densitom 5:343–353
Fujita T, Fujii Y, Goto B (1999) Measurement of forearm bone in children by peripheral computed tomography. Calcif Tissue Int 64:34–39
Macdonald HM, Kontulainen SA, Mackelvie-O’Brien KJ, Petit MA, Janssen P, Khan KM, McKay HA (2005) Maturity- and sex-related changes in tibial bone geometry, strength and bone-muscle strength indices during growth: a 20-month pQCT study. Bone 36:1003–1011
Moyer-Mileur L, Xie B, Ball S, Bainbridge C, Stadler D, Jee WS (2001) Predictors of bone mass by peripheral quantitative computed tomography in early adolescent girls. J Clin Densitom 4:313–323
Neu CM, Manz F, Rauch F, Merkel A, Schoenau E (2001) Bone densities and bone size at the distal radius in healthy children and adolescents: a study using peripheral quantitative computed tomography. Bone 28:227–232
Neu CM, Rauch F, Manz F, Schoenau E (2001) Modeling of cross-sectional bone size, mass and geometry at the proximal radius: a study of normal bone development using peripheral quantitative computed tomography. Osteoporos Int 12:538–547
Rauch F, Neu C, Manz F, Schoenau E (2001) The development of metaphyseal cortex—implications for distal radius fractures during growth. J Bone Miner Res 16:1547–1555
Rauch F, Schoenau E (2005) Peripheral quantitative computed tomography of the distal radius in young subjects—new reference data and interpretation of results. J Musculoskelet Neuronal Interact 5:119–126
Schoenau E, Neu CM, Rauch F, Manz F (2001) The development of bone strength at the proximal radius during childhood and adolescence. J Clin Endocrinol Metab 86:613–618
Wang Q, Alen M, Nicholson P, Lyytikainen A, Suuriniemi M, Helkala E, Suominen H, Cheng S (2005) Growth patterns at distal radius and tibial shaft in pubertal girls: a 2-year longitudinal study. J Bone Miner Res 20:954–961
Bechtold S, Ripperger P, Bonfig W, Pozza RD, Haefner R, Schwarz HP (2005) Growth hormone changes bone geometry and body composition in patients with juvenile idiopathic arthritis requiring glucocorticoid treatment: a controlled study using peripheral quantitative computed tomography. J Clin Endocrinol Metab 90:3168–3173
Binkley T, Johnson J, Vogel L, Kecskemethy H, Henderson R, Specker B (2005) Bone measurements by peripheral quantitative computed tomography (pQCT) in children with cerebral palsy. J Pediatr 147:791–796
Brennan BM, Mughal Z, Roberts SA, Ward K, Shalet SM, Eden TO, Will AM, Stevens RF, Adams JE (2005) Bone mineral density in childhood survivors of acute lymphoblastic leukemia treated without cranial irradiation. J Clin Endocrinol Metab 90:689–694
Heap J, Murray MA, Miller SC, Jalili T, Moyer-Mileur LJ (2004) Alterations in bone characteristics associated with glycemic control in adolescents with type 1 diabetes mellitus. J Pediatr 144:56–62
Moyer-Mileur LJ, Dixon SB, Quick JL, Askew EW, Murray MA (2004) Bone mineral acquisition in adolescents with type 1 diabetes. J Pediatr 145:662–669
Quick JL, Ward KA, Adams JE, Mughal MZ (2006) Cortical bone geometry in asthmatic children. Arch Dis Child 91:346–348
Rauch F, Land C, Cornibert S, Schoenau E, Glorieux FH (2005) High and low density in the same bone: a study on children and adolescents with mild osteogenesis imperfecta. Bone 37:634–641
Reilly SM, Hambleton G, Adams JE, Mughal MZ (2001) Bone density in asthmatic children treated with inhaled corticosteroids. Arch Dis Child 84:183–184
Roth J, Palm C, Scheunemann I, Ranke MB, Schweizer R, Dannecker GE (2004) Musculoskeletal abnormalities of the forearm in patients with juvenile idiopathic arthritis relate mainly to bone geometry. Arthritis Rheum 50:1277–1285
Schwahn B, Rauch F, Wendel U, Schonau E (2002) Low bone mass in glycogen storage disease type 1 is associated with reduced muscle force and poor metabolic control. J Pediatr 141:350–356
Schweizer R, Martin DD, Schwarze CP, Binder G, Georgiadou A, Ihle J, Ranke MB (2003) Cortical bone density is normal in prepubertal children with growth hormone (GH) deficiency, but initially decreases during GH replacement due to early bone remodeling. J Clin Endocrinol Metab 88:5266–5272
Engelke K, Gluer CC (2006) Quality and performance measures in bone densitometry: part 1: errors and diagnosis. Osteoporos Int 17:1283–1292
Gilsanz V (1998) Bone density in children: a review of the available techniques and indications. Eur J Radiol 26:177–182
Schoenau E, Neu CM, Beck B, Manz F, Rauch F (2002) Bone mineral content per muscle cross-sectional area as an index of the functional muscle-bone unit. J Bone Miner Res 17:1095–1101
Schiessl H, Ferretti J, Tysarczyk-Niemeyer G, Willnecker J (1996) Noninvasive bone strength index as analyzed by peripheral computed tomography (pQCT). In: Schoenau E (ed) Paediatric osteology: new developments in diagnostics and therapy. Elsevier Science B.V., Amsterdam, pp 141–146
Burr DB, Turner CH (2003) Biomechanics of bone. In: Favus MJ (ed) Primer on the metabolic bone diseases and disorders of mineral metabolism. The American Society for Bone and Mineral Research, Philadelphia, pp 58–64
National Osteoporosis Society (2004) A practical guide to bone densitometry in children. Camerton, Bath, UK
Watson SJ, Jones AL, Oatway WB, Hughes JS (2005) Ionising radiation exposure of the UK Population: 2005 review. Health Protection Agency Centre for Radiation, Chemical and Environmental Hazards Radiation Protection Division, Chilton, Didcot, Oxfordshire, UK
Lettgen B, Neudorf U, Hosse R, Peters S, Reiners C (1996) Bone density in children and adolescents with rheumatic diseases. Preliminary results of selective measurement of trabecular and cortical bone using peripheral computerized tomography. Klin Padiatr 208:114–117
Zemel B, Bass S, Binkley T, Ducher G, Macdonald H, McKay H, Moyer-Mileur L, Shepherd J, Specker B, Ward K, Hans D (2008) Peripheral quantitative computed tomography in children and adolescents: the 2007 ISCD Pediatric Official Positions. J Clin Densitom 11:59–74
Moyer-Mileur LJ, Quick JL, Murray MA (2008) Peripheral quantitative computed tomography of the tibia: pediatric reference values. J Clin Densitom 11:283–294
Ward KA, Ashby RL, Roberts SA, Adams JE, Zulf Mughal M (2007) UK reference data for the Hologic QDR Discovery dual-energy x ray absorptiometry scanner in healthy children and young adults aged 6–17 years. Arch Dis Child 92:53–59
Phillimore P, Beattie A, Townsend P (1994) Widening inequality of health in northern England, 1981–91. BMJ 308:1125–1128
Census Dissemination Unit (2001) Census Aggregate Outputs [Online] Available: http://www.census.ac.uk/cdu/2001/ [Accessed August 2005]
Cole TJ, Freeman JV, Preece MA (1995) Body mass index reference curves for the UK, 1990. Arch Dis Child 73:25–29
Freeman JV, Cole TJ, Chinn S, Jones PR, White EM, Preece MA (1995) Cross sectional stature and weight reference curves for the UK, 1990. Arch Dis Child 73:17–24
Stratec Medizintechnik GmbH (2004) XCT 2000 Manual Software Version 5.50
Cole TJ, Green PJ (1992) Smoothing reference centile curves: the LMS method and penalized likelihood. Stat Med 11:1305–1319
Ashby RL (2006) Growth and development of the skeleton in normal children. Unpublished PhD thesis, The University of Manchester
Slemenda CW, Reister TK, Hui SL, Miller JZ, Christian JC, Johnston CC Jr (1994) Influences on skeletal mineralization in children and adolescents: evidence for varying effects of sexual maturation and physical activity. J Pediatr 125:201–207
Leonard MB, Shults J, Elliott DM, Stallings VA, Zemel BS (2004) Interpretation of whole body dual energy X-ray absorptiometry measures in children: comparison with peripheral quantitative computed tomography. Bone 34:1044–1052
Ward KA, Adams JE, Hangartner TN (2005) Recommendations for thresholds for cortical bone geometry and density measurement by peripheral quantitative computed tomography. Calcif Tissue Int 77:275–280
van Staa TP, Bishop N, Leufkens HG, Cooper C (2004) Are inhaled corticosteroids associated with an increased risk of fracture in children? Osteoporos Int 15:785–791
Muller ME, Webber CE, Bouxsein ML (2003) Predicting the failure load of the distal radius. Osteoporos Int 14:345–352
Wilhelm G, Felsenberg D, Bogusch G, Willnecker J, Thaten J, Gummert P (1999) Biomechanical examinations for validation of the bone strength strain index SSI, calculated by peripheral quantitative computed tomography. In: Lyritis GP (ed) Musculoskeletal interactions II. Hylonome, Athens, pp 105–108
Horikoshi T, Endo N, Uchiyama T, Tanizawa T, Takahashi HE (1999) Peripheral quantitative computed tomography of the femoral neck in 60 Japanese women. Calcif Tissue Int 65:447–453
Di Leo C, Tarolo GL, Bagni B, Bestetti A, Tagliabue L, Pietrogrande L, Pepe L (2002) Peripheral quantitative Computed Tomography (PQCT) in the evaluation of bone geometry, biomechanics and mineral density in postmenopausal women. Radiol Med (Torino) 103:233–241
Fricke O, Sumnik Z, Tutlewski B, Stabrey A, Remer T, Schoenau E (2008) Local body composition is associated with gender differences of bone development at the forearm in puberty. Horm Res 70:105–111
Macdonald H, Kontulainen S, Petit M, Janssen P, McKay H (2006) Bone strength and its determinants in pre- and early pubertal boys and girls. Bone 39:598–608
Roth J, Linge M, Tzaribachev N, Schweizer R, Kuemmerle-Deschner J (2007) Musculoskeletal abnormalities in juvenile idiopathic arthritis—a 4-year longitudinal study. Rheumatology (Oxford) 46:1180–1184
Ward KA, Roberts SA, Adams JE, Mughal MZ (2005) Bone geometry and density in the skeleton of pre-pubertal gymnasts and school children. Bone 36:1012–1018
Marjanovic E, Ward K, Adams J (2008) The impact of accurate positioning on measurements made by peripheral QCT in the distal radius. Osteoporos Int [Epub ahead of print], Nov 4
Rauch F, Tutlewski B, Fricke O, Rieger-Wettengl G, Schauseil-Zipf U, Herkenrath P, Neu CM, Schoenau E (2001) Analysis of cancellous bone turnover by multiple slice analysis at distal radius: a study using peripheral quantitative computed tomography. J Clin Densitom 4:257–262
Rauch F, Travers R, Munns C, Glorieux FH (2004) Sclerotic metaphyseal lines in a child treated with pamidronate: histomorphometric analysis. J Bone Miner Res 19:1191–1193
Davies JH, Gregory JW (2003) Radiographic long bone appearance in a child administered cyclical pamidronate. Arch Dis Child 88:854
Smith SA, Norris BJ (2004) Changes in the body size of UK and US children over the past three decades. Ergonomics 47:1195–1207
Carter DR, Bouxsein ML, Marcus R (1992) New approaches for interpreting projected bone densitometry data. J Bone Miner Res 7:137–145
Molgaard C, Thomsen BL, Prentice A, Cole TJ, Michaelsen KF (1997) Whole body bone mineral content in healthy children and adolescents. Arch Dis Child 76:9–15
Rauch F, Glorieux FH (2004) Osteogenesis imperfecta. Lancet 363:1377–1385
Boyde A, Travers R, Glorieux FH, Jones SJ (1999) The mineralization density of iliac crest bone from children with osteogenesis imperfecta. Calcif Tissue Int 64:185–190
Rauch F (2006) Material matters: a mechanostat-based perspective on bone development in osteogenesis imperfecta and hypophosphatemic rickets. J Musculoskelet Neuronal Interact 6:142–146
Acknowledgements
The authors would like to thank the research participants and their families, the schools where recruitment was undertaken, our dedicated team of radiographers and database manager Mr. Mike Machin.
We would like to gratefully acknowledge financial support from the Central Manchester and Manchester Children’s University Hospital NHS Research Endowment Fund and the support of the National Osteoporosis Society (Camerton, Bath, UK), which awarded Rebecca Ashby a Linda Edwards Memorial Studentship in 2003 and funded the initial part of the study (1997–1998).
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
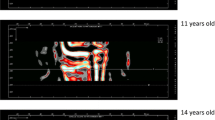
Patient example
This pre-pubertal male with osteogenesis imperfecta (OI) type I had a history of low trauma fractures of the long bones from 14 months of age. He had also suffered minor fractures of the toes and fingers. At 11 years of age, he complained of non-specific back pain; subsequent radiographs revealed anterior wedge fractures of two thoracic vertebrae. He underwent bone densitometry assessment DXA and pQCT at 11.5 years of age.
For clinical assessments of all patients attending the Manchester Metabolic Bone Disease Clinic, we measure patients’ height and weight and calculate SDS age from United Kingdom reference data [35, 36]. DXA is used to measure the lumbar vertebrae (L1–L4) to provide measurements of lumbar spine (LS) bone area (square centimetre) and bone mineral content (BMC) (grams per square centimetre) [32]. LS bone mineral apparent density (BMAD) is calculated [57]. The three-stage algorithm of Molgaard [58] is used to determine whether a patient has ‘short’ (i.e. height for age), ‘narrow’ (i.e. lumbar spine bone area for height) or ‘light’ (i.e. LS BMC for LS bone area) bones at the lumbar spine; SDS are calculated [32]. pQCT is used to measure the 4% distal radius to provide measurements total and trabecular BMD, as suggested by the recent International Society for Clinical Densitometry guidelines [30]. SDS are calculated for total and trabecular BMD according to age.
Measurement | Value | SDS |
Heighta for age | 133 cm | −1.9 |
Weighta for age | 32.6 kg | −0.7 |
Lumbar spine BMAD for age | 0.18 g/cm3 | −3.2 |
Lumbar spine bone area for height | 30.33 cm2 | −3.9 |
Lumbar spine BMC for lumbar spine bone area | 9.60 g | −2.9 |
Total BMDa for age | 192.1 mg/cm3 | −3.2 |
Trabecular BMDa for age | 116.3 mg/cm3 | −2.5 |
Clinical interpretation of anthropometric, DXA lumbar spine and pQCT distal radius total and trabecular BMD
This patient has reduced height for age (SDS −1.9), indicating he has small bones. He also has narrow (SDS −3.9) and light (SDS −2.9) bones and reduced LS BMAD (SDS −3.2). This suggests that he has impaired lumbar spine bone growth and mineralisation, secondary to his OI [32]. At the distal radius, the total and trabecular BMD are low due to fewer and thinner trabeculae, as well as thinner cortical shell in OI [59].
We also use pQCT to provide a number of non-clinical measurements at the 50% mid-shaft radius diaphysis in order to gain a greater insight into how disease or treatment may affect bone geometry, strength and muscle. We use pQCT to provide measurements of cortical thickness, cortical BMC, the polar strength strain index (polar SSI) and axial moment of inertia (AMI) at the 50% mid-shaft radius. This is in accordance with those which the ISCD suggest be measured at a diaphyseal site [30]. In addition, we also use pQCT to measure cortical area, bone area and cross-sectional muscle area of the 50% mid-shaft radius. As height has a strong correlation with cortical bone parameters [40] and is a powerful determinant of cortical bone geometry and strength [31, 41], we calculate SDS for all variables measured at the 50% mid-shaft radius by height. In addition, we calculate SDS for cortical BMC by age.
Measurement | Value | SDS |
Cortical thicknessa for height | 1.7 mm | −0.9 |
Cortical BMCa for age | 37.6 mg/mm | −2.8 |
Cortical BMCa for height | 37.6 mg/mm | −1.8 |
Polar SSIa for height | 70.7 mm3 | −2.0 |
AMIa for height | 193.0 mm4 | −2.4 |
Cortical area for height | 33.9 mm2 | −2.3 |
Bone area for height | 52.6 mm2 | −2.3 |
Cross-sectional muscle area for height | 1139.5 mm2 | 0.0 |
Interpretation of BMC, bone geometry, strength and muscle parameters at the 50% mid-shaft radius according to height and cortical BMC according to age
At the mid-shaft radius, adaption to higher bone material property in OI [60] results in the smaller bone area (SDS −2.3) and cortical area, which can lead to a reduction in long-bone strength (polar SSI SDS −2.0 and AMI SDS −2.4) in patients with OI [61]. Whilst this patient has reduced cortical parameters for his height, he has normal cross-sectional muscle area suggesting that bone strength of his slender long-bone diaphyses are not appropriately adapted to loading from his forearm muscles [61].
Taking into consideration the clinical, radiological and bone densitometry findings, the patient was commenced on cyclical three monthly infusions of pamidronate (3-amino-1-hydroxypropylidene-1,1-bisphosphonate) in order to reduce his risk of fractures at appendicular and axial skeletal sites.
Rights and permissions
About this article
Cite this article
Ashby, R.L., Ward, K.A., Roberts, S.A. et al. A reference database for the Stratec XCT-2000 peripheral quantitative computed tomography (pQCT) scanner in healthy children and young adults aged 6–19 years. Osteoporos Int 20, 1337–1346 (2009). https://doi.org/10.1007/s00198-008-0800-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-008-0800-2