
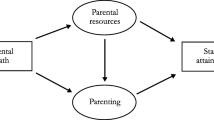
Abstract
Using Austrian administrative data, this study examines the causal effect of parental death on daughters’ fertility through a difference-in-differences approach. The findings indicate that parental death leads to quantitatively insignificant changes in the number of children and the probability of childlessness. Complementary analyses show no substantial effects on labor market participation, residential mobility, or long-term mental health. The evidence suggests that fertility decisions remain largely unaffected by the logistical and emotional challenges of parental loss, highlighting the resilience of reproductive choices to external life shocks.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
1 Introduction
The death of a parent is a profound life event, often accompanied by emotional and practical challenges that can reshape various aspects of an individual’s life. In particular, fertility decisions may be affected by the loss of informal childcare, changes in mental health, or shifts in economic circumstances. Yet, the extent to which parental death influences fertility remains unclear.
Parental death may influence fertility decisions in complex and potentially conflicting ways. On one hand, the loss of informal childcare and financial support from parents could raise the costs of raising children, leading to a reduction in fertility. Bereavement-related declines in mental health might also discourage childbearing by shifting focus away from family planning. On the other hand, parental death could alleviate responsibilities for elderly care and improve economic stability through inheritance, potentially increasing fertility by freeing up time and resources, offsetting some negative impacts. However, given the multifaceted influences on human decision-making, where personal circumstances, cultural norms, and economic considerations coalesce in shaping demographic patterns in the course of human history (Galor 2022), such external shocks may ultimately have a limited effect on fertility decisions, especially if the perceived long-term benefits of having children outweigh the immediate challenges.
We demonstrate that parental death has little to no statistically significant effect on daughters’ fertility. Estimating the effects up to five years after the first death of a parent, we find some statistically significant, yet quantitatively insignificant changes in the cumulative number of children and the probability of being childless. In the years following parental death, our point estimates imply a 1.58 percent decrease in the cumulative number of children and a 1.34 percent increase in the probability of being childless. In the context of the existing literature on fertility, we consider this effect size to be rather limited. Even when considering the 95 percent confidence interval, we can rule out a decrease in the cumulative number of children larger than 3.43 percent and an increase in the probability of being childless larger than 2.37 percent. Besides this, we do not find a statistically significant change in either the overall probability of giving birth or in the probability of having a first-, second-, third-, or fourth- and higher-order birth. We present a series of complementary analyses that further substantiate our finding of a limited fertility response. First, we show that parental death does not lead to a reduction in daughters’ number of children in a scenario where this would be most expected, namely when the loss of informal childcare is particularly pronounced. There is no fertility effect if the mother dies, or the daughter resides in an area with low availability of formal childcare. Second, the absence of effect heterogeneity by the age of the daughter, the deceased parent, and the surviving parent further confirms the robustness of our findings. Third, we find consistent effects on complementary outcomes. One would expect changes in fertility to be reflected in changes in labor market outcomes. Consistent with a rather small effect on fertility, we find that parental death does not impact women’s labor market participation. Moreover, there is no change in daughters’ place of residence, which could be affected by caregiving responsibilities for the surviving parent. Although we find a short-term deterioration in mental health, this does not seem to translate into substantial changes in major life decisions, of which fertility is arguably one of the most important.
We utilize comprehensive administrative data from Austria and link daughters with their parents. The Austrian Social Security Database (Zweimüller et al 2009) covers all private sector employees and includes information on live births and death years, which we use to define our main outcome and treatment variable. Additionally, it provides detailed information on socio-economic characteristics, labor market histories, and earnings for both daughters and their parents. We link this with detailed health record data from the Upper Austrian Health Insurance Fund, which provides us with information on outpatient visits, prescribed medication, and hospital visits.
To identify the causal effect of parental death on daughters’ fertility, we implement a quasi-experimental method similar to Fadlon and Nielsen (2019, 2021). We construct a counterfactual for daughters who experience their first parental death during reproductive age by pairing those who lose a parent in a given year with daughters who do so exactly a fixed number of years later. The estimation sample, therefore, only includes daughters who all experience the death of a parent. This should result in greater comparability between daughters in the treatment and control group compared to using daughters who do not experience a parental death during reproductive age as controls. Under the parallel trends assumption, we can estimate the causal treatment effect in a difference-in-differences framework. To assess the plausibility of the parallel trends assumption, we estimate a dynamic difference-in-differences model to determine whether there already are statistically significant trends before the treatment. We conduct several robustness analyses to support the validity of our identification strategy. We restrict the sample to sudden parental deaths, include different control variables, specify different numbers of years between actual parental death in the treatment and control group, and construct an alternative control group from the large pool of daughters who do not lose a parent during reproductive age using nearest-neighbor matching.
Evidence on the impact of parental death on adult children’s fertility is rather limited, and existing studies are primarily correlational, providing mixed results.Footnote 1,Footnote 2 While some studies find an increase in fertility (Beaujouan and Solaz 2023; Rackin and Gibson-Davis 2022), others find a decrease (Del Boca 2002; Jensen and Zhang 2023; Okun and Stecklov 2021). Some find no impact or mixed results (Dahlberg 2020; Kertzer et al. 2009). Most studies are based on survey data, often with small sample sizes, or cannot establish a causal effect of parental death on adult children’s fertility. For the US, Rackin and Gibson-Davis (2022) find that maternal death is associated with a higher likelihood of first birth. For France, Beaujouan and Solaz (2023) show that a maternal death during childhood is associated with higher completed fertility of women. For Italy, Del Boca (2002) shows that women with living parents are more likely to have children. In contrast, Kertzer et al. (2009) find no association between parental death and the transition to first and second birth.Footnote 3
The studies by Okun and Stecklov (2021); Dahlberg (2020), and Jensen and Zhang (2023) are most closely related to our work. They either use administrative data sources and/or employ a causal identification strategy.Footnote 4 Okun and Stecklov (2021)’s study is based on census and administrative data from Israel. Using individual fixed effects, the authors find that parental death is associated with a reduction in the five-year birth probability by around five percentage points. The effects are larger when the parents live in the same locality as their children and if already existing grandchildren are under six years old. Dahlberg (2020) uses data from the Swedish population register and applies survival analysis to show that a parental death during reproductive age affects the probability of a first birth predominantly in the short run. While it increases for younger individuals, there is generally a negative effect for those older than 23. Parental death is also associated with a higher likelihood of being childless at age 45. Jensen and Zhang (2023) utilize administrative data from Denmark and nearest-neighbor matching combined with difference-in-differences to analyze the effect of parental death on adult children’s employment and earnings. In their mechanism analysis, they additionally show the impact of parental death on the total number of children and find a slight reduction for both men and women within five years following death.
We contribute to the existing literature in four ways. First, we add additional evidence utilizing a credible identification strategy to estimate the causal effect of parental death on daughters’ fertility. Previous studies have mainly used non-causal methods like simple linear regression with control variables (Beaujouan and Solaz 2023), survival analysis (Dahlberg 2020; Kertzer et al. 2009), or individual fixed effects regressions (Del Boca 2002; Okun and Stecklov 2021; Rackin and Gibson-Davis 2022). Since the fertility trajectories of children with and without deceased parents tend to be different (see Fig. 1), and other papers remain silent about these differences, their results are potentially biased. We use women who experience parental death a few years apart as controls in a difference-in-differences setting and show that our comparison involves women who are on similar fertility trends before the parental death. A recent exception from the use of non-causal empirical strategies is Jensen and Zhang (2023) which uses nearest-neighbor matching combined with difference-in-differences. Their main focus, however, is on labor market outcomes. We add by analyzing different fertility margins, providing effect heterogeneity, and a detailed discussion of pre-trends.
Second, we provide suggestive evidence against the informal childcare channel, which is one of the main mechanisms through which parental death could theoretically reduce fertility. Previous studies have emphasized the importance of informal childcare by grandparents (e.g., Okun and Stecklov 2021; Rutigliano 2023). Nevertheless, we demonstrate that the death of a parent has little to no effect on daughters’ fertility, even in situations where the loss of informal childcare should be particularly pronounced.

Comparing fertility trends of daughters with and without parental death
Third, we strengthen the plausibility of our main result by analyzing the effect of parental death on relevant complementary outcomes. For this, we combine several high-quality administrative data sources, allowing us to consider additional outcomes that are related to fertility and/or the loss of a parent. These include labor supply, the place of residence, and mental health. Previous studies tend to use survey data (e.g., Beaujouan and Solaz 2023; Rackin and Gibson-Davis 2022) or administrative data for fertility only (e.g., Dahlberg 2020; Okun and Stecklov 2021).Footnote 5 We also focus on the fertility effect of parental death while additionally providing results on other important life decisions of women within a coherent empirical analysis.
Fourth, we add evidence for Austria to the literature, which has previously shown mixed results in countries with diverse institutional settings. We show that parental death has little to no effect on fertility in a Central European country with rather conservative gender norms and limited availability of nurseries.
Our work also complements the literature on the effects of parental health events on other outcomes. Studies in this area have documented the health consequences of parental death (e.g., Appel et al. 2016; Böckerman et al. 2023; Fadlon and Nielsen 2019; Frimmel et al. forthcoming; Glaser and Pruckner 2023; Jensen and Zhang 2023; Kristiansen 2021; Leopold and Lechner 2015; Marks et al. 2007) as well as the effects on labor market outcomes (e.g., Frimmel et al. forthcoming; Jensen and Zhang 2023; Marcos 2023; Norén 2020; Rellstab et al. 2020). Negative effects of parental death have also been established for other outcomes, especially when parental death is experienced during childhood. These include worse educational outcomes (e.g., Kailaheimo-Lönnqvist and Erola 2020; Kailaheimo-Lönnqvist and Kotimäki 2020; Kristiansen 2021), an increase in the likelihood to commit violent crimes (e.g., Berg et al. 2019; Wilcox et al. 2010) and higher mortality (e.g., Hiyoshi et al. 2021; Rostila and Saarela 2011).
As the death of parents inherently reduces parental support, our results also speak to the literature on the role of parental support in determining fertility.Footnote 6 Rutigliano (2023) uses information on whether a woman’s mother is alive as an instrument for parental availability and finds that increased parental availability raises the probability of having a second birth. Other research using retirement reforms (e.g., Aparicio-Fenoll and Vidal-Fernandez 2015; Battistin et al. 2014; Eibich and Siedler 2020; Ilciukas 2023), distance measures (e.g., Pink 2018), or expected future childcare provision (e.g., Pessin et al. 2022; Rutigliano 2020) as instruments for parental availability tends to find that higher availability increases fertility. We differ from these studies by analyzing the overall effect of parental death, instead of focusing only on parental availability, which is only one potential channel influencing daughters’ fertility.
The remainder of this paper is structured as follows. Section 2 describes the institutional setting and data sources used to construct our analysis sample. Section 3 outlines the empirical strategy and discusses the main identifying assumptions. Section 4 presents the results. Finally, Section 5 concludes the paper.
2 Institutional setting and data
2.1 Institutional setting
Fertility: Fertility has fallen below the replacement rate in many developed countries (Okun and Stecklov 2021). Austria is no exception to this trend. Panel a of Fig. A.1 in the Supplementary Material shows the total fertility rate for Austria since 1950. From 2.5 live births per woman in the mid-1960s, the rate has declined steadily ever since, leveling off at around 1.5. A similar pattern can be observed for other European countries and the United States, although in the latter, the fertility rate peaked earlier and has stabilized at a higher level.
At the same time, the average age at birth in Austria has increased (see Panel b of Fig. A.1 in the Supplementary Material). The average age at birth was 27.1 years in 1990 and 31.3 years in 2020. The increase in age at first birth is even greater. While women were, on average, 25 years old when they gave birth to their first child in 1990, they were on average 30 years in 2020. Subsequent generations of parents, therefore, become older as their children enter reproductive age. Meanwhile, the likelihood of losing a parent increases with the age of the children (see Fig. A.2 in the Supplementary Material). This implies that the experience of losing a parent during this important stage in an individual’s life has become more common. One in four women in our data have lost at least one parent before the age of 45, making it a common experience.
Social security and health insurance: Austria’s Bismarckian social security system provides universal access to high-quality healthcare as well as pension, disability, and unemployment benefits for the entire population. Health insurance is offered by various funds, with more than 99 percent of the population covered. The association with one particular health insurance fund is determined by an individual’s place of residence and occupation. The Austrian Health Insurance Fund (Österreichische Gesundheitskasse) is the largest insurer, covering almost 75 percent of all private sector workers.Footnote 7 Health insurance for children is provided through their parents and spouses can be co-insured with their partners (Ahammer et al. 2021).
The mandatory health insurance covers all forms of healthcare, including visits to general practitioners (GPs) and specialists in the outpatient sector, inpatient care, and prescription drugs, with little or no copayments.Footnote 8 The system is primarily financed by wage-based social security contributions from employers and employees. While expenditures in the outpatient sector (including medication) are mainly financed through these contributions, hospitalization costs are also partly covered by tax revenues. GPs provide primary care and can refer patients to specialists and/or a hospital if necessary. As the first point of access to the healthcare system, GPs traditionally function as gatekeepers (Ahammer et al. 2021; Glaser and Pruckner 2023).
The social security system also provides paid maternity and parental leave. Paid maternity leave is compulsory and extends to eight weeks before and eight weeks after the birth of a child. The duration of subsequent parental leave depends on whether both parents take time off (35 weeks) or only one parent uses parental leave (28 weeks) (Ahammer et al. 2023).
Gender norms and formal childcare: Regarding attitudes toward family and gender roles, Austria is a rather conservative country. Panel c of Fig. A.1 in the Supplementary Material supports this claim by showing data on gender norms from the International Social Survey Programme. One in five Austrians strongly agrees with the statement that preschool children suffer when their mother works. In a more egalitarian country like Denmark, the corresponding proportion is only 5 percent. Similarly, 18 percent of Austrians believe that family life as a whole suffers through a working mother. This share is significantly lower in other countries, ranging from 2 percent in Norway to 12 percent in France. These more conservative views are also reflected in a higher share of part-time work among Austrian women (33.1 percent) than among Danish women (23.1 percent) (Ahammer et al. 2023).
Compared to other EU countries, enrollment in formal childcare in Austria is relatively low, especially for children under three. According to data from Eurostat, about 23 percent of Austrian children under the age of three spend at least one hour per week in formal childcare. This is well below the EU-27 average of 35.8 percent. Apart from the rather conservative gender norms, this is also due to the limited availability of nurseries (especially in rural areas) (Ahammer et al. 2023). The situation is different for children between the ages of three and six. In this age group, only 8.1 percent of children in Austria are not in formal childcare, which is lower than the EU-27 average of 11.6 percent (see Eurostat). Nevertheless, grandparents are important providers of informal childcare in Austria. As Panel d of Fig. A.1 in the Supplementary Material shows, 60 percent of Austrians think that family members should be the primary providers of childcare. This share is well below 50 percent in other European countries, like France, Norway, Denmark, and Sweden. Analyzing survey data, Kaindl and Wernhart (2012) show that in Austria around 45 percent of households receive informal childcare from grandparents at least several times a month if the youngest child is under six years old. Consequently, the role of grandparents in childcare appears to be important in the Austrian setting.
2.2 Data sources and sample construction
Data sources: To estimate the effect of parental death on the subsequent fertility of daughters, we need to link three generations. The first generation is the parents, the second generation is their daughters, and the third generation is the potential grandchildren.Footnote 9 We use comprehensive administrative data from Austria that allow us to link the generations. Information on live births of daughters and death years of parents can be obtained from the Austrian Social Security Database (ASSD), which is available for all Austrian private sector employees and their dependents from 1972 to 2018 (Zweimüller et al 2009). These data also provide information on socio-economic characteristics, labor market histories, and earnings.
The social security data can be linked to detailed health record data from the Upper Austrian Health Insurance Fund (UAHIF), which covers more than one million private sector employees and their dependents in Upper Austria from 2005 to 2018.Footnote 10 We can use detailed information on outpatient visits, prescribed medications, and hospital visits. In addition, the data provide information on the place of residence on the postal code level, which allows us to estimate effect heterogeneity depending on the driving distance between parents and their daughters. Based on the place of residence, we can also add information on the availability of formal childcare facilities, which has been obtained from Statistics Austria.
Sample construction: Using the data described above, we link all daughters included in the social security data to both of their parents and construct an unbalanced panel at the daughter-year level. The information on the parents includes their year of death, which allows us to identify the death of the first parent.Footnote 11 Since we are conditioning on the death of the first parent, we start with a sample of daughters whose parents are alive at the beginning of the sample period. We use only daughters who experience their first parental death between the ages of 25 and 44 for our main empirical specification, which is described in detail in Section 3. In a robustness check, we use daughters who have not yet experienced parental death as controls to demonstrate that our results are independent of the control group.
To obtain the set of observations relevant to answering the research question, we restrict the sample in the following ways: Since we are studying fertility, we restrict the sample to include only observations during reproductive age. Thus, we only include periods when daughters are between 20 and 44 years old. In addition, we only include parental deaths that occurred between 2000 and 2018.
2.3 Outcome variables
Fertility: We use a binary indicator that is one if a daughter had a live birth in a given year and zero otherwise. The binary indicator is based on the ASSD data, which records specific spells for live births (Anzeige einer Lebendgeburt). The social security records only live births, and therefore, no information on abortions, miscarriages, and stillbirths is available. Since we also observe children’s birth years, we can define distinct indicators for first-, second-, and higher-order births. By adding up the binary indicator over time for each daughter, we can examine the cumulative number of children as an outcome.
Additional outcomes: This study also considers the effect of parental death on daughters’ mental health, labor market outcomes, and living conditions. We use a binary indicator for antidepressant prescriptions (N06A) to measure changes in mental health. The labor market outcomes are based on the ASSD data. We selected the number of days in employment, the number of days in unemployment, and the yearly wage as relevant outcome variables.Footnote 12 Lastly, we also use the information on daughters’ and parents’ places of residence on the postal code level to study potential changes in living conditions. We compute the driving time between the postal code centroid of the daughter and the postal code centroid of the survivor to see whether the surviving parent lives closer to their daughter after the death. We also consider the daughters’ probability of living in the same postal code area as before the parental death. Note that the mental health and location outcomes are based on the health record data, which is only available for Upper Austria. Therefore, we only analyze these outcomes for daughters residing in Upper Austria. Our main fertility outcome and the labor market outcomes are studied for women residing in Austria.
3 Empirical strategy
3.1 Main estimation strategy
The objective of this study is to estimate the causal effect of a parent’s death on their daughters’ fertility. Finding an appropriate control group to evaluate this effect is challenging. A naïve approach would be to simply compare the fertility of women who have lost a parent with those who have not. This approach is problematic because women who experience the death of their parents may have very different characteristics and fertility trajectories than women with living parents. Figure 1 demonstrates that this is indeed the case. Panel a displays the raw age trends of the annual birth probability of women with a parent dying and women without a parental death during reproductive age in our data. Compared to the latter group, women in the former group tend to give birth at a younger age (20 to 25 years) and are less likely to give birth in their late twenties and thirties. These differential fertility trajectories are also evident in Panel b, where we display the probability of giving birth from five years before the parents’ death to four years after. To obtain the necessary data structure for women without parental death during reproductive age, a placebo death year is randomly assigned.Footnote 13 Women who lose a parent are more likely to give birth in the years before parental death and less likely to do so afterward when compared with women who do not lose a parent. Additionally, the fertility trends between the two groups are completely different. Daughters with and without a parental death also differ substantially in other key characteristics. The comparison in Table A.1 shows that affected daughters are about 2.4 years older than unaffected daughters, earn about 1.4 thousand Euros more per year, and have higher hospital, outpatient, and medication expenditures. Table A.2 in the Supplementary Material shows that the differences in daughters’ age and the socio-economic status of daughters and their parents are important determinants of the difference in the probability of giving birth before the parental death.
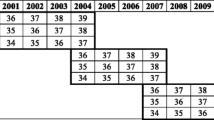
To obtain an appropriate counterfactual for women who experience the death of a parent and to estimate the causal effect of parental death on daughters’ subsequent fertility, we implement a quasi-experimental method similar to Fadlon and Nielsen (2019, 2021). We restrict the sample to daughters of childbearing age exposed to their first parental death and then utilize the exact timing of the death in a dynamic difference-in-differences framework. Restricting the sample this way ensures that daughters are in a life stage in which fertility decisions are made and that their parents die at an age at which they would take on the role of an active grandparent. Figure 2 illustrates the construction of the treatment and control group. Daughters who are affected by parental death in year d are paired with control daughters who experience the death exactly \(\tau \) years later. In our baseline specification, we set \(\tau \) = 5, meaning that daughters in the control group are assigned a placebo death in year d, while their parent actually passes away in d + 5. This matching approach is repeated for each death year d for which valid control daughters are found within our sample period.Footnote 14 To increase the power of the analysis, the same women may be in both the treatment and control group, but a woman never serves as a control for herself. By constructing our sample in this way, we can estimate treatment effects up to four years after parental death, as control daughters are themselves treated in d + 5.

After constructing the treatment and control group, we estimate the following model:
where \(y_{itd}\) is the outcome variable observed for daughter i in calendar year t who experiences the (placebo) parental death in year d. d is the actual death year of the parent for daughters in the treatment group and five years before the actual parental death year for daughters in the control group. \(Death_{id}\) is a binary indicator equal to one if the parent of daughter i dies in d and equal to zero if the parent of daughter i dies in d + 5. \(1(\cdot )\) are a series of indicator variables for the individual years relative to the (placebo) parental death. \(\delta _{l}\) denotes the treatment effects of interest relative to the reference period of two years before the (placebo) death. \(\textbf{X}_{itd}\) is a set of control variables that include fixed effects for daughters’ age, the year of the (placebo) parental death, and the parental age at (placebo) death. In particular, these control variables account for the age trend in the outcome variable, which is important when analyzing fertility. The results in Table A.3 in the Supplementary Material show that the inclusion of different control variables does not change the results. Since the death of a parent may affect multiple daughters of one family, we cluster the standard errors at the family level.
To identify the causal effect, it is necessary to assume that the fertility behavior of daughters in the treatment and the control group would have evolved in parallel in the absence of the death of their parent. Throughout this study, we use the dynamic DiD specification to inspect for non-differential pre-trends. A potential threat to the parallel trend assumption is a fertility adjustment in anticipation of parental death (e.g., due to a preceding deterioration in parental health). We address this concern with a series of tests. First, in all our estimations, we set the baseline period to two years before the (placebo) parental death. This allows us to estimate treatment effects for the year prior to the parental death and to test for the existence of anticipation effects. Second, anticipation effects should be less of a concern if the death of a parent is less foreseeable for daughters. Therefore, we also estimate the effects for different sub-samples that include only sudden deaths in Section 4.4. These results are qualitatively similar to our main results. Third, we demonstrate the robustness of our findings by altering the value of \(\tau \). The identification strategy imposes a trade-off between the comparability of the experimental groups and the possible length of the analysis period. A smaller \(\tau \) results in a shorter time difference between the actual parental death in the treated and control group, which should lead to greater similarity in daughters’ observable and unobservable characteristics, as well as in expectations about parental death. A larger \(\tau \) allows us to analyze a longer time period, but the daughters in the treatment and control groups tend to become less comparable. Lastly, constructing a control group as described by Fadlon and Nielsen (2019, 2021) has the advantage that all daughters in the sample are ultimately affected by the death of a parent but are so only a few years apart.Footnote 15 This implies that daughters in the treatment and control group should be more comparable than in other event study methods that use daughters who do not lose a parent as a control group. Indeed, Fig. 3 shows that the differences in observable characteristics between the treatment and control group are smaller in our main sample compared to an alternative sample that uses daughters who do not experience the death of a parent as controls (see also Table 1 and Table A.1 in the Supplementary Material). This could also mean that expectations about their parents’ future health, for example, should be more similar in our treatment and control group than in this alternative setting. Overall, the absence of statistically significant effects in the year before parental death and the results of the analyses described above suggest that anticipation does not appear to be a major factor in our setting.

Comparing variable balancing across methods. Note—This compares the balancing of different observable characteristics for three possible methods of constructing the control group. These methods are described in detail in Section 3. The box plots illustrate the distribution of the standardized differences (measured in percent) reported in Column 5 of Tables 1, A.7 and A.1. The standardized difference is defined as the difference in means between the treated and control group for a given variable (\(\mu _{treated} - \mu _{control})\) divided by the average standard deviation\(\left( \sqrt{0.5\cdot (\sigma ^2_{treated} + \sigma ^2_{control})} \right) \) and multiplied by 100. All box plots exclude values that lie 1.5 times the interquartile range below the first quartile or 1.5 times the interquartile range above the third quartile (i.e., outside values)
Another potential threat to identification is that differences in parents’ socio-economic status are systematically related to parental age at death and daughters’ fertility patterns. Although daughters and parents are on average the same age at the time of the (placebo) treatment, the construction of the control group implies that parents in the control group are \(\tau \) years older when they actually die compared to parents in the treatment group. This older age at death might be the result of a higher socio-economic status, which could be related to the fertility decisions of their daughters. As Table A.4 in the Supplementary Material shows, parents in the treatment group have a lower average yearly wage than parents in the control group. To address this concern, we implement the following steps. First, Column 6 of Tables A.3, A.5, and A.6 in the Supplementary Material show the results when we additionally control for the deceased parent’s average yearly wage, which should measure socio-economic status. The results are qualitatively similar to our main findings. Second, we show in Fig. A.3 in the Supplementary Material that the difference in parents’ socio-economic status is smaller compared to our main specification when using a smaller value of \(\tau \). As described above, we find similar effects of parental death on daughters’ fertility when setting \(\tau \) to 3. Third, we find similar results when restricting the sample to sudden deaths. The fact that parents in the treatment group die at an earlier age could be related to their lower socio-economic status, which could in turn mean that their deaths are more likely due to individual lifestyle factors. If we restrict the sample to sudden deaths only (e.g., to parents with low healthcare expenditures before parental death), the health status of parents in the treatment and control group should be more similar. This could also reduce the differences in socio-economic status. Indeed, Fig. A.3 in the Supplementary Material shows that differences in parents’ average yearly wages are smaller for the different definitions of sudden deaths.
Table 1 presents descriptive statistics comparing the characteristics of daughters in the treatment and control group before the (placebo) death of the parent. The daughters are approximately 30 years old at the time of the (placebo) parental death, work 247 days per year, and earn about 21 thousand Euros per year. Before the death of their parent, women in the treatment group had 0.015 more children, worked 1.3 days less per year, and earned 35 cents less per day than the women in the control group. Treated women spend approximately 20 Euros more on medication per year. There are no statistically significant differences between the two groups for all other health-related variables. Although there are some differences between daughters in the two groups, we regard most of these differences to be quantitatively insignificant. Table A.4 in the Supplementary Material shows descriptive statistics comparing the characteristics of the dying parents in the treatment and control group before their (placebo) death. Parents in the treatment group are 0.35 years older at (placebo) death, have fewer days of employment (18.2), more days in retirement (18.6), and lower average yearly lifetime wages (1,000 Euros). In addition, total healthcare expenditures and the likelihood of receiving care allowance are higher in the treatment group. The gender composition is quite well-balanced. Although the health status of the dying parent appears to deteriorate already before death, we are confident that this does not affect our results. In Section 4.4, we analyze sudden deaths as a robustness check and arrive at the same qualitative conclusions. Anticipation therefore does not seem to play a major role in our setting.

Histograms. Note—This shows histograms of selected discrete variables for daughters in our main estimation sample. The distributions are plotted separately for daughters in the treatment group (gray bars) and the control group (hollow black bars). Detailed information on the construction of the treatment and control group is provided in Section 3. a shows the distribution of the year of the first parental death for treated daughters and the assigned placebo death year for control daughters. The actual years of the first parental death are shown in b. The distributions of the daughters’ birth years and current age are shown in c and d. e and f show the distribution of the birth years and the age at the (placebo) death of the dying parent
Figure 4 shows histograms of relevant variables by treatment status. The year of the (placebo) parental death is distributed similarly between treated and control women (Panel a), as are daughters’ birth years (Panel c). This implies that also daughters’ age at the (placebo) parental death is similarly distributed between the two groups. The current age of the daughters (Panel d), the birth years of the dying parents (Panel e), and the age of the parent at (placebo) death (Panel f) also follow identical distributions in the treatment and control group. As implied by setting \(\tau \) = 5, the distribution of the years of the actual parental deaths is shifted by five years for the control group (Panel b). Figure A.4 in the Supplementary Material shows that the balancing in these histograms is also similar when using a sample without overlap. In this case, a woman can be in either the treatment or the control group, but not in both.
3.2 Robustness check: propensity score matching
In our main empirical specification, we only analyze women who all lose a parent during the sample period. An alternative control group would be women without a parental death who are otherwise similar in key observable characteristics. For this, we use the large potential pool of daughters who do not lose a parent during reproductive age to construct a control group by applying nearest-neighbor matching. We perform the matching separately for each birth year of daughters to ensure that the age distribution is the same for treated and matched daughters. The propensity score is computed using several demographic and labor market characteristics of daughters and their parents. For daughters, the variables include the first and last year of observation, a binary indicator for whether the daughter has siblings, the number of children, the yearly wage, and binary indicators for blue- and white-collar employment. For their mothers and fathers, we use the birth year, the yearly wage, and binary indicators for blue-collar employment, white-collar employment, and retirement. All variables are measured when the daughters are 24 years old.Footnote 16 Each treated daughter is matched with five nearest neighbors.Footnote 17 These nearest neighbors are then assigned the year of the parental death of the respective treated daughter to construct a placebo event time.Footnote 18 Panels a and b of Fig. A.5 in the Supplementary Material show that there are only small differences between the propensity scores of treated and matched daughters, indicating very close matches. Table A.7 and Fig. A.6 in the Supplementary Material show descriptive statistics and histograms for the matched sample. All key observable characteristics are closely balanced for daughters in the treatment and the control group.
We then use this alternative sample to estimate the effect of parental death in the following dynamic difference-in-differences design:
where \(y_{it}\) is the outcome variable observed for daughter daughter i in calendar year t. \(Death_{i}\) is equal to one if the parent of daughter i loses a parent and equal to zero if both parents are alive during reproductive age. \(1(\cdot )\) are indicator variables representing the individual years relative to the (placebo) parental death. \(\delta _{l}\) denotes the treatment effects of interest relative to the reference period two years before the (placebo) parental death. \(\textbf{X}_{it}\) includes the same set of control variables as in Eq. 1. Standard errors are again clustered on the family level.
In Fig. 3, we compare the balancing of key observable characteristics between the treatment and control group for the different ways of constructing the control group: our main empirical specification based on Fadlon and Nielsen (2019, 2021), the matched sample of daughters who do not experience a parental death, and the naïve control group of all daughters without a parental death. The results show that the naïve control group has the worst balancing, while our preferred method performs similarly to the matched sample of women without parental death. However, using daughters who experience death exactly \(\tau \) years in the future as controls has an additional advantage. This approach is more likely to balance both observable and unobservable characteristics, given that all daughters are treated only a few years apart.

Comparing the number of children of daughters in the treatment and control group. Note—This shows the cumulative number of children for daughters included in our main estimation sample. The cumulative number of children is plotted separately for daughters in the treatment group (blue diamonds) and the control group (gray dots). The definition of the treatment and control group is described in Section 3. a plots the number of children as a function of age. b compares the average number of children for five years before and four years after the parental death. Zero indicates the year of the parental death. The shaded areas represent 95 percent confidence intervals

Dynamic effect of parental death on daughters’ fertility. Note—This shows the estimated coefficients with 95 percent confidence intervals for the effect of parental death on different fertility margins. All estimates are based on Eq. 1. a shows the change in the cumulative number of children. The estimates can be interpreted as the change in the cumulative number of children in a given year. b uses a binary indicator that is one if the cumulative number of children is zero in a given year and zero otherwise as an outcome. The estimates can thus be interpreted as the percentage point change in the probability of being childless in a given year. c shows the change in birth probability. The estimates can be interpreted as the percentage point change in the annual birth probability. Estimates are shown for five years before and five years (including the year of the parental death) after the parental death. Zero indicates the year of the parental death. The relative period \(-\)2 has been chosen as a reference period. The number of observations and the mean of the outcome variable for treated daughters in the reference period are reported in the bottom right corner. Standard errors are clustered on the family level
4 Results
This section presents the findings of our study. First, we show in Section 4.1 how the death of the parents affects the fertility of their daughters. Section 4.2 discusses effect heterogeneity. We provide results on the effect of parental death on complementary outcomes in Section 4.3. Finally, Section 4.4 presents the results of several robustness checks.
4.1 Effect of parental death on daughters’ fertility
Number of children and childlessness: In a first step, we provide a descriptive analysis of the number of children in the treatment and control group of our main estimation sample. Figure 5 presents the unadjusted number of children as a function of age in Panel a and as a function of the time relative to the parental death in Panel b (where zero represents the year of the parental death). The average number of children, including 95 percent confidence intervals, is plotted separately for women who experience the death of a parent (treatment) and for women who are affected \(\tau =5\) years later (control). The confidence intervals in Panel a clearly overlap, indicating that there are no statistically significant differences in fertility patterns between the two groups across the age distribution. Panel b suggests that the difference in the number of children between treated and control daughters is slightly smaller after the parental death than before, although the confidence intervals of both lines overlap.
Expanding on this descriptive analysis, we estimate the dynamic causal effect of parental death on daughters’ fertility following Eq. 1. The results are presented in Fig. 6, which shows the point estimates for five years before and after the parental death together with 95 percent confidence intervals. The graph displays the treatment effects in relation to the two years preceding the death on the vertical axis. The horizontal axis marks the years relative to the death of the first parent. Again, zero indicates the year of death. Panels a and b show the estimated coefficients for the effect of parental death on the cumulative number of children and the probability of being childless. The cumulative number of children decreases by 0.0086 children in the year of the parental death. This corresponds to a reduction of around 1.58 percent. The coefficients in all other post-periods are not statistically significant. The probability of being childless increases by 0.59 to 0.86 percentage points in the years following the death of a parent. Given the probability of being childless two years before the parental death of around 0.643, the coefficients would suggest an increase by 0.92 to 1.34 percent. For both outcomes, all estimated coefficients in the time period before the parental death are statistically insignificant. This suggests that the parallel trend assumption is not violated.
Birth probability: Figure 6c shows the estimated coefficients for the effect of parental death on daughters’ annual birth probability. There is no statistically significant effect over the entire five-year post-death period. When considering the 95 percent confidence interval, we can rule out an increase larger than 0.009 percentage points in period 1 and a reduction smaller than 0.009 percentage points in period 0. Compared to the mean of 0.072 this translates to a maximal and minimal effect of 12.5 percent. However, from period 2 onward the point estimates become substantially smaller. All estimated coefficients in the time period before the parental death are statistically insignificant. This suggests that the parallel trend assumption is not violated.
As just demonstrated, there is no evidence to suggest that the death of a parent affects a woman’s probability of giving birth. However, the birth indicator used so far does not account for the number of children a woman already has, making it difficult to measure changes in birth probability by birth order. The death of a parent could potentially affect the extensive and intensive margin of fertility differently. Given that the decision to have any children at all is possibly one of the most important in an individual’s life, the death of a parent might only have a small influence on this decision. However, it may have a larger effect on the decision to have additional children, which can be more dependent on external factors such as the availability of informal childcare by grandparents. To investigate whether the death of a parent has a varying impact on the extensive and intensive margins of fertility, Fig. 7 a, b, c, and d displays the estimated coefficients for the effect of parental death on the probability of having a first-, second-, third-, or fourth- or higher-order birth.Footnote 19 There is no statistically significant effect of parental death on any of these outcomes. Table A.8 in the Supplementary Material provides the coefficients for all fertility outcomes.
Discussion: We find a small reduction in the number of children by 1.58 percent and a small increase in the probability of being childless by 1.34 percent. The effect sizes are also similar when only focusing on women between the ages of 25 and 35, i.e., a sample where the risk of having children is likely to be very high (see Fig. A.7 in the Supplementary Material). Further, parental death does not lead to a statistically significant change in daughters’ overall probability of giving birth as well as the probability of having a first-, second-, third-, or fourth- or higher-order birth. Although we find some statistically significant effects, they lack quantitative significance compared to findings in the existing literature on parental death and fertility. Dahlberg (2020) find a peak increase in the first birth risk of 14 percent for women. The risk of being childless at age 45 increases by 18.65 percent for men and by 12.68 for women percent if one parent dies. Rackin and Gibson-Davis (2022) show that maternal deaths are associated with a 62 percent increase in the probability of first birth. Jensen and Zhang (2023) find that parental death reduces the total number of children by 0.003 to 0.012 (0.193 to 0.773 percent), which is in line with our finding that the cumulative number of children decreases by a quantitatively insignificant amount of no more than 0.0086 after the death of a parent.

Dynamic effect of parental death on daughters’ other fertility margins. Note—This shows the estimated coefficients with 95 percent confidence intervals for the effect of parental death on different fertility margins. All estimates are based on Eq. 1. For the results in a, b, c, and d, we defined four separate binary indicators that are one if a daughter had a first-, second-, third-, or fourth- or higher-order birth in a given year. The estimates in these panels can thus be interpreted as the percentage point change in the annual probability of having a first-, second-, third-, or fourth- or higher-order birth, respectively. Estimates are shown for five years before and five years (including the year of the parental death) after the parental death. Zero indicates the year of the parental death. The relative period \(-\)2 has been chosen as a reference period. The number of observations and the mean of the outcome variable for treated daughters in the reference period are reported in the bottom right corner. Standard errors are clustered on the family level

Effect of parental death on daughters’ cumulative number of children by age. Note—This shows the estimated average coefficients with 95 percent confidence intervals for the effect of parental death on daughters’ cumulative number of children by different age categories. a and b estimate Eq. 1 separately for each daughter age at (placebo) death and then compute the arithmetic mean of coefficients. c and d split the sample by the age of the parent responsible for the (placebo) parental death at the time of the (placebo) parental death. e and f estimate the effects separately by the age of the surviving parent at the time of the (placebo) death of the other parent. a, c, and e show the average coefficients for the years after parental death (relative periods 0 to 4). b, d, and f show the average coefficients for the years preceding the parental death (relative periods \(-\)5 to \(-\)1, excluding the baseline period \(-\)2), where hollow (full) circles indicate that the p-value of the F-test for the joint significance of all pre-treatment coefficients is above (below) 0.05. The estimates can be interpreted as the average change in the number of children in a given year. The estimation sample includes five years before and five years (including the year of the parental death) after the parental death. The relative period \(-\)2 has been chosen as a reference period. Standard errors are clustered on the family level
To provide further context to our results, we also provide the percentage impact on fertility for a small selection of studies cited in the literature review by Hart et al. (2023). In Norway, public childcare expansions increased fertility by 44 percent. In Austria, the extension of parental leave from 12 to 24 months increased the birth probability by 5.7 to 14 percent. A German parental leave reform increased the annual birth probability by 16 percent. A reform that increased direct financial transfers in Canada increased fertility by 12 percent.
Overall, the comparison with the closely related literature and also broader literature suggests that our finding of a small reduction in the number of children appears to be quantitatively insignificant.
4.2 Effect heterogeneity
We have shown that, on average, the death of a parent has little to no effect on women’s fertility. In this section, we show that this is the case even in settings where the loss of informal childcare should be particularly prominent. For this, we evaluate the effects separately based on the age of the daughter and parents at the time of death, whether the mother or the father dies, the presence of siblings, and the availability of formal childcare facilities. Additionally, this analysis strengthens the validity of our main results by presenting the robustness in different subgroups.
Age at death: To assess the heterogeneity with respect to the age of the daughter at the time of the parental death, we estimate Eq. 1 separately for ages at death ranging from 25 to 39 years. We then compute the average pre- and post-period coefficients and plot the results for the number of children in Fig. 8. Panel a shows that none of the average post-treatment coefficients are statistically significant. Panel b presents the corresponding average coefficients in the pre-period to verify the validity of the parallel trend assumption. We do not observe statistically significant effects on the number of children in either age group in the years preceding the parental death (except at age 38). We perform a similar exercise by partitioning the sample based on the age at death of the parent (Panels c and d) and by the age of the surviving parent at the time of the death of the other parent (Panels e and f). Nearly all of the estimated average post-period coefficients are statistically insignificant. We repeat the same exercises for the probability of being childless and the birth probability. Figures A.8 and A.9 in the Supplementary Material show the results. As virtually none of the average post-treatment coefficients are statistically significant, we do not find heterogeneity in the effect of parental death on the probability of being childless and the birth probability with respect to the age of the daughters, the deceased parents, and the survivors. All these results suggest that women do not change their fertility behavior in response to parental death, regardless of the age.
Gender of deceased parent: We also estimate the dynamic effect of parental death on daughters’ fertility by distinguishing between the gender of the deceased parent. Panel a of Fig. 9 and Fig. A.10 in the Supplementary Material shows the results for the number of children and the probability of being childless. For both outcomes, we find no statistically significant effects when the mother dies. When the father dies, there is a small decrease in the number of children and a corresponding increase in the probability of being childless. The magnitude of these effects is similar to the full sample estimates. Since the confidence intervals of the estimates for both groups overlap, we cannot reject the null hypothesis that the effects are identical in both groups. Panel a of Fig. A.11 in the Supplementary Material shows the results for the birth probability, which indicate that the estimated effects on the probability of giving birth are not statistically significant for either subgroup.

Dynamic effect of parental death on daughters’ cumulative number of children by the intensity of the loss of informal childcare. Note—This compares the estimated coefficients with 95 percent confidence intervals for the effect of parental death on daughters’ cumulative number of children for different subgroups with varying intensity of the loss of informal childcare. Estimates are based on Eq. 1. a shows the effects separately for daughters whose mothers die (gray diamonds) and for daughters whose fathers die (blue circles). b differentiates between daughters with siblings (gray diamonds) and without siblings (blue circles). In c, we estimated the effects separately for daughters living in postal code areas with above-median (gray diamonds) and below-median (blue circles) availability of formal childcare. The estimates can be interpreted as the change in the cumulative number of children in a given year. Estimates are shown for five years before and five years (including the year of the parental death) after the parental death. Zero indicates the year of the parental death. The relative period \(-\)2 has been chosen as a reference period. The number of observations and the mean of the outcome variable for treated daughters in the reference period are reported in the bottom right corner. Standard errors are clustered on the family level
Siblings: Panel b of Fig. 9 and Fig. A.10 in the Supplementary Material shows the treatment effects separately for women with and without siblings. The full sample results are driven by daughters with siblings. There is no statistically significant effect on the number of children and the probability of being childless for women without siblings. Again, the confidence intervals of the estimates for both groups overlap. Panel b of Fig. A.11 in the Supplementary Material shows the results for the birth probability. Parental death does not have a statistically significant effect on the birth probability in any period after death for either group.
Formal childcare: We also estimate the effect of parental death on daughters’ fertility separately for daughters located in areas with above- and below-median availability of formal childcare.Footnote 20 The results are presented in Fig. 9c and in Panel c of Figs. A.10 and A.11 in the Supplementary Material. As the place of residence is only available for women who are insured in Upper Austria, this analysis is limited to this subgroup. We find no statistically significant effects of parental death on the number of children, the probability of being childless, and the birth probability for women with both high and low access to formal childcare.
Discussion: Overall, the results of the heterogeneity analyses support our main finding that the death of a parent has little to no statistically significant effect on daughters’ fertility. Considering the number of children, we find a small decrease of similar magnitude to the full sample results for daughters whose fathers die and for daughters with siblings. For these groups, we also find a corresponding increase in the probability of being childless. For all other subgroups analyzed, including daughters with low availability of formal childcare and maternal deaths, none of the estimated coefficients are statistically significant. Additionally, we do not find significant treatment effects on daughters’ probability of giving birth in any of the studied subgroups. There are no effects observed for different age groups, whether the mother or father dies, whether a daughter has siblings or not, and whether formal childcare is readily available or not.
These results offer suggestive evidence against one of the main ways in which parental death could theoretically decrease fertility, which is the absence of informal childcare provided by parents after their death. We do not observe a decrease in fertility in situations where the loss of informal childcare should be particularly pronounced: First, informal childcare is predominantly provided by grandmothers (see, e.g., Hank and Buber 2009), so one would expect to find a negative fertility effect when the mother dies. However, we do not find a fertility response in this case. Second, siblings could support mothers with the provision of childcare, so fertility would decline if one does not have siblings.Footnote 21 However, the fertility of women without siblings is not affected. Third, women living in areas with low availability of formal childcare facilities might find it difficult to compensate for the loss of informal childcare after parental death. However, we do not find a decline in fertility among women living in such areas.
4.3 Effect on complementary outcomes
So far, we have shown that the death of a parent has little to no effect on daughters’ fertility. This is the case even in situations in which the loss of informal childcare should be particularly prominent. To set the absence of a quantitatively relevant fertility effect into a broader context, we now analyze complementary outcomes that should be related to fertility and/or the death of a parent. These include labor market outcomes, place of residence, and mental health.
Several studies have shown a negative relationship between childbirth and women’s labor supply (e.g., Angelov et al. 2016; Kleven et al. 2019). One would, therefore, expect that an increase in fertility would translate into a decrease in labor supply and vice versa. Our comprehensive administrative data provide the opportunity to study the impact of a parent’s death on various labor market outcomes. Figure 10 displays the results of this analysis. Panel a shows the effect on yearly days of employment, Panel b shows yearly days of unemployment, and Panel c shows yearly wages. The results show that the death of a parent does not have a statistically significant effect on any of these outcomes. Given the existing evidence on the relationship between childbearing and women’s labor supply, our finding of little to no fertility response to parental death is consistent with the absence of a labor market response.
Apart from labor supply, the place of residence is another essential decision. In addition, the death of a parent might induce changes in the daughters’ place of residence to care for the surviving parent. To analyze this, we use the health record data, which also provides information on individuals’ place of residence at the postal code level for women and surviving parents insured in Upper Austria. Figure 11a illustrates the impact of parental death on the driving duration between the home location of daughters and surviving parents in minutes.Footnote 22 Panel b displays the probability that the distance is greater than ten minutes.Footnote 23 Panel c shows the probability of a daughter having the same postal code as two years before the parental death. There are no statistically significant effects on distance measures and women’s probability of living in the same area. This suggests that parental death does not trigger a change in the place of residence (and labor supply), which makes the absence of a substantial effect on an even more important life decision such as fertility plausible.

Dynamic effect of parental death on daughters’ labor market outcomes. Note—This shows the estimated coefficients with 95 percent confidence intervals for the effect of parental death on selected labor market outcomes of daughters. The estimates are based on Eq. 1. a shows the effects on the annual number of employment days, and b on the number of unemployment days. c shows the impact on the yearly wage. The yearly wage is based on the social security contribution basis. Estimates are shown for five years before and five years (including the year of the parental death) after the parental death. Zero indicates the year of the parental death. The relative period \(-\)2 has been chosen as a reference period. The number of observations and the mean of the outcome variable for treated daughters in the reference period are reported in the bottom right corner. Standard errors are clustered on the family level

Dynamic effect of parental death on distance between daughter and survivor. Note—This shows the estimated coefficients with 95 percent confidence intervals for the effect of parental death on the geographical distance between daughters and surviving parents. The estimates are based on Eq. 1. a shows the effects on the average driving duration between daughters and parents in minutes, and b shows the probability that this duration is above 10 min. For these outcome variables, we used information on daughters’ and parents’ place of residence on the postal code level. We first geocoded the postal codes with the help of the R-package opencage to obtain the coordinates of the respective postal code centroids. The driving duration between the postal code centroids has been computed using the R-package osrm. c shows the effect on the probability that a daughter lives in the same postal code area as two years before the parental (placebo) death. The results are based on a binary indicator that is one if a daughter’s postal code in a given year is the same as in the reference period \(-\)2 and zero otherwise. Note that all estimates are based on daughters insured in Upper Austria as we can observe the place of residence only for this group. While in a and b, we require daughters and parents to be insured in Upper Austria, c only requires daughters to be insured in Upper Austria and places no such restriction on their parents. Estimates are shown for five years before and five years (including the year of the parental death) after the parental death. Zero indicates the year of the parental death. The relative period \(-\)2 has been chosen as a reference period. The number of observations and the mean of the outcome variable for treated daughters in the reference period are reported in the bottom right corner. Standard errors are clustered on the family level
The lack of a substantial impact on fertility and other life decisions could also be because the death of the parents has no disruptive effect on women. We investigate this claim by estimating the dynamic treatment effect of parental death on the use of antidepressants for the subsample of women insured in Upper Austria. The results are presented in Fig. 12. The probability of receiving an antidepressant prescription increases sharply by 1.9 percentage points in the year of the parent’s death. The effect is statistically significant at the five percent level. The increase in antidepressant use is around 36 percent compared to the average pre-period prescription probability of 5.3 percent. The effect remains similar in the year after the death and then disappears in the following years. This finding indicates that the death of a parent leads to a short-term deterioration in mental health, implying that parental death indeed affects daughters. However, this does not translate into substantial changes in important life decisions, such as labor supply, place of residence, and ultimately fertility.
4.4 Robustness
Sudden deaths: It could be the case that the parents’ health is worsening before death and therefore daughters in the treatment group may adjust their fertility accordingly. To address the concerns regarding non-similar expectations of daughters in the treatment and control group, we construct different samples in which it is more likely that daughters have similar expectations about the death of their parents. We aim to identify sudden deaths in three different ways. First, the dying parent’s total healthcare expenditures before death are below the median. One would expect below-median healthcare utilization to be associated with more unexpected deaths. Second, the dying parent did not receive care allowance before death.Footnote 24 Third, the cause of death is likely to be unexpected. We define sudden death causes as diseases of the circulatory system, cancers with a low survival probability, and accidents.

Dynamic effect of parental death on daughters’ mental health. Note—This shows the estimated coefficients with 95 percent confidence intervals for the effect of parental death on the prescription probability for antidepressants (ATC N06A) of daughters insured in Upper Austria. The estimates are based on Eq. 1. Note that all estimates are based on daughters insured in Upper Austria as we can observe healthcare expenditures only for this group. Estimates are shown for five years before and five years (including the year of the parental death) after the parental death. Zero indicates the year of the parental death. The relative period \(-\)2 has been chosen as a reference period. The number of observations and the mean of the outcome variable for treated daughters in the reference period are reported in the bottom right corner. Standard errors are clustered on the family level

Parents’ total healthcare expenditure before death for sudden deaths. Note—This shows the development of total healthcare expenditures of the parent responsible for the parental death in the five years leading up to the death and the year of the death. The sample only includes observations from the treatment group. Because healthcare data are only available for individuals insured in Upper Austria, this sample includes only daughters whose parents are insured in Upper Austria. The gray dots show the average total healthcare expenditures in each period for all parents in the treatment group. The blue hollow symbols differentiate between different definitions of sudden deaths. The blue hollow diamonds represent parents whose average total healthcare expenditures before death are below the sample median. Total healthcare expenditures include hospital, outpatient, and medication expenditures. The average is computed based on the year of the parental death and the two years preceding it. The blue hollow squares represent parents who received no care allowance before death. The sample only includes (placebo) parental deaths until 2012, as the information on care allowance is only available until 2012. The blue hollow triangles represent parents who died due to a sudden death cause. Sudden death causes include all deaths due to injuries, poisoning and certain other consequences of external causes (ICD-10 chapter XIX), diseases of the circulatory system (ICD-10 chapter IX), and cancers with a low survival probability (malignant neoplasm of esophagus (ICD-10 C15), malignant neoplasm of liver and intrahepatic bile ducts (ICD-10 C22), malignant neoplasm of pancreas (ICD-10 C25), malignant neoplasm of bronchus and lung (ICD-10 C33), malignant neoplasm of trachea (ICD-10 C34), and malignant neoplasm of brain (ICD-10 C71)). Information on death causes is only available until 2009. Because information on healthcare expenditures is only available after 2005, there are no observations for relative period \(-\)5 in this group. Zero indicates the year of the parental death. The shaded areas represent 95 percent confidence intervals
Figure 13 shows the patterns of total healthcare expenditures for the dying parent in the treatment group in the years before their death for the different definitions of unexpected deaths and for our main sample. In our main sample, parents’ healthcare expenditures increase before death, as would be expected. From \(-\)4 to \(-\)2, there is a moderate increase, but from \(-\)2 onward, healthcare expenditures rise quite steeply. This implies that there are at least two years before death in which daughters have the opportunity to adjust their fertility. In the samples without care allowance recipients and only sudden death causes, healthcare expenditures do not begin to rise until two years before death, so that anticipation is reduced. If parents’ healthcare expenditures are below the median, there is no increase in expenditures before death and the death should thus be unexpected. Therefore, daughters should be even less likely to anticipate their parent’s death and adjust fertility accordingly than in the other two samples.

Dynamic effect of parental death on daughters’ fertility outcomes for sudden deaths. Note—This shows the estimated coefficients with 95 percent confidence intervals for the effect of parental death on different fertility margins for different definitions of sudden deaths. All estimates are based on Eq. 1. a shows the change in the cumulative number of children. b uses a binary indicator that is one if the cumulative number of children is zero in a given year and zero otherwise as an outcome. c shows the change in birth probability. Estimates are shown for five years before and five years (including the year of the parental death) after the parental death. Zero indicates the year of the parental death. The relative period \(-\)2 has been chosen as a reference period. Standard errors are clustered on the family level. We use three different definitions of sudden deaths: First, we only use daughters’ where the average total healthcare expenditures of the parent responsible for the (placebo) parental death is below the sample median. Total healthcare expenditures include hospital, outpatient, and medication expenditures. The average is computed based on the year of the (placebo) parental death and the two years preceding it. Because healthcare data are only available for individuals insured in Upper Austria, this sample includes only daughters whose parents are insured in Upper Austria. Second, we estimate the effects for daughters whose parent did not receive care allowance at any point before the (placebo) parental death. The sample only includes (placebo) parental deaths until 2012, as the information on care allowance is only available until 2012. Third, we only keep parents with a sudden death cause. Sudden death causes include all deaths due to injuries, poisoning and certain other consequences of external causes (ICD-10 chapter XIX), diseases of the circulatory system (ICD-10 chapter IX), and cancers with a low survival probability (malignant neoplasm of esophagus (ICD-10 C15), malignant neoplasm of liver and intrahepatic bile ducts (ICD-10 C22), malignant neoplasm of pancreas (ICD-10 C25), malignant neoplasm of bronchus and lung (ICD-10 C33), malignant neoplasm of trachea (ICD-10 C34), and malignant neoplasm of brain (ICD-10 C71)). Information on death causes is only available until 2009
Figure 14 shows the effects of parental death on daughters’ fertility for the different definitions of unexpected deaths (see also Table A.9 in the Supplementary Material). When considering the number of children and the probability of childlessness, the results are quantitatively similar to our main analysis. For some definitions of sudden deaths, the results even suggest that there are no statistically significant effects. For all our definitions, which tend to capture exogenous sudden parental deaths, we do not find statistically significant effects on daughters’ birth probability. The coefficients in the pre-period are also not statistically significant. Overall, this analysis is reassuring as it suggests that anticipation does not seem to play a major role in our setting. Analyzing sudden deaths, we reach the same conclusion of little to no statistically significant effect of parental death on daughters’ fertility.
Other robustness checks: Our main result of little to no statistically significant effect on daughters’ fertility is further supported by the following analyses: (i) the inclusion of different control variables, (ii) the choice of different levels of \(\tau \) in the construction of the control group in our main estimation method, (iii) using an alternative control group of matched daughters who did not experience the death of a parent, (iv) the use of a sample without overlap, (v) restricting the sample to daughters insured in Upper Austria, and (vi) restricting the sample to a fully balanced panel. We discuss each analysis in detail below.
First, we estimate the dynamic treatment effect of parental death on daughters’ fertility using various sets of control variables. The results are presented in Tables A.3, A.5, and A.6 in the Supplementary Material. Column 1 shows the results without any additional control variables, while Columns 2 to 4 gradually include the main control variables. In Column 5, we control for the age at death of both mothers and fathers separately instead of only controlling for the age at death of the deceased parent. Column 6 adds the logarithm of the deceased parent’s average yearly lifetime wage as an additional control variable. We add a calendar year fixed effect in Column 7 and control flexibly for daughters’ age at death in Column 8. As a last alternative specification in Column 9, we estimate a standard two-way fixed effects model, controlling for daughters’ age. As one daughter can appear both in the treated and the control group, the usual individual fixed effect is defined as an individual-times-treated fixed effect. The results for the number of children and the probability of being childless are stable across the different specifications. Regardless of the chosen control variables, we do not find any statistically significant treatment effect for the birth probability in the post-death period in any of the eight specifications.

Robustness: alternative control groups. Note—This shows the estimated coefficients with 95 percent confidence intervals for the effect of parental death on daughters’ cumulative number of children. a shows the estimates from Eq. 1 for different specifications of \(\tau \) in the construction of the control group. b shows the estimates from Eq. 2. In this specification, daughters who do not lose a parent are paired with daughters who do so based on nearest-neighbor matching (see Section 3 for details). The blue dots show the point estimates for this sample, while the gray diamonds represent the coefficients from our main specification in Fig. 6a. All estimates can be interpreted as the change in the cumulative number of children in a given year. Estimates are shown for five years before and up to seven years (including the year of the parental death) after the parental death in a and for five years after the parental death in b. Zero indicates the year of the parental death. The relative period \(-\)2 has been chosen as a reference period. The number of observations and the mean of the outcome variable for treated daughters in the reference period are reported in the bottom right corner. Standard errors are clustered on the family level
Second, we assess the sensitivity of our results to the choice of \(\tau \) in constructing the control group. The selection of \(\tau \) represents a trade-off between the number of follow-up periods that can be analyzed and the comparability between the treatment and control group. A larger \(\tau \) allows for more years in the post-treatment period, while a smaller \(\tau \) results in greater comparability between the groups. In our baseline specification, we set \(\tau \) = 5. Panel a of Figs. 15 and A.12 in the Supplementary Material demonstrate the robustness of our main findings to different levels of \(\tau \). The estimated coefficients remain similar in magnitude and statistical significance when \(\tau \) is set to three, five, or seven.
Third, we demonstrate that our results are robust to the choice of the control group. So far, we have only considered daughters who all experience the death of a parent during reproductive age and have exploited the different timing of these deaths to construct the control group. An alternative control group would be those daughters who do not lose a parent during their reproductive age. To ensure the comparability between these two groups of daughters, we match them on key observable characteristics as outlined in Section 3. We then estimate the dynamic treatment effect using Eq. 2. The estimates for the effect of parental death on the number of children are shown in Fig. 15b. Again, we find negative coefficients in all post-treatment periods. Although the point estimates are slightly larger in magnitude than those from our main specification, the confidence intervals of both estimates clearly overlap in all periods.Footnote 25 The patterns of the other fertility margins are also similar to our main empirical strategy (see Fig. A.13 in the Supplementary Material).
Fourth, the results are robust to the use of a sample without overlap.Footnote 26 In this case, a woman can be in either the treatment or the control group, but not in both. Table 2 shows the effects of parental death on different fertility outcomes using the sample without overlap. We do not find any statistically significant effects on any fertility outcome, further supporting our main finding of little to no statistically significant effect on daughters’ fertility. Table A.10 in the Supplementary Material shows descriptive statistics and Fig. A.4 in the Supplementary Material shows histograms of relevant variables by treatment status.
Fifth, we show that our results remain unchanged when restricting the sample to daughters insured in Upper Austria. As some of the variables used in the analysis (e.g., healthcare expenditures and driving distances) can only be observed for this subgroup, we estimate Eq. 1 for all fertility outcomes for daughters insured in Upper Austria. The estimates reported in Table A.11 in the Supplementary Material show that there is no statistically significant change in the number of children and the probability of being childless in any of the five years following the parental death. The coefficients for the probability of having a birth are also not statistically significant. Again, the absence of an effect is independent of the birth order.
Finally, we show that our results remain unchanged when using a fully balanced panel. Figure A.14 shows the dynamic effect of parental death on daughters’ probability of being observed in the sample using our main empirical strategy. The average probability of being observed in the sample in the pre-period is 96.8 percent. After parental death, this probability increases by around 0.5 percentage points. To address potential concerns about the small increase in the likelihood of being observed in the sample, Fig. A.15 shows the effects on our main outcome variables using a fully balanced panel in which attrition is zero per construction. One can see that attrition does not affect the main results.
5 Discussion and conclusions
Based on high-quality administrative data from Austria, we implement a credible identification strategy exploiting the timing of deaths in a difference-in-differences design to estimate the causal effect of parental death on daughters’ fertility. The number of children decreases by 1.58 percent, and the probability of being childless increases by 1.34 percent, but there is no effect on daughters’ probability of giving birth in a given year. The number of children can be considered a measure of daughters’ total fertility, while birth probability tends to capture the timing of their fertility. This suggests that we find a small decline in total fertility that does not seem to be reflected in changes in fertility timing. These divergent results may arise because a single birth can only be captured in the year the birth occurs, but not in the subsequent years when analyzing birth probability. Given that we observe only a small decline in daughters’ number of children and this decline may not be clustered in any specific year after parental death, it may be difficult to capture this statistically using birth probability as an outcome.
Throughout this study, our findings consistently indicate a limited fertility response to parental death. Although we find statistically significant effects, they lack quantitative significance compared to the findings in the existing fertility literature. We do not find a reduction in daughters’ number of children in a scenario where this would be most expected, namely when the loss of informal childcare is particularly pronounced. Furthermore, we do not find effect heterogeneity by the age of the daughter, the deceased parent, and the surviving parent. In line with a rather limited effect on fertility, the death of a parent does not induce reactions in daughters’ labor supply. Nor does it change daughters’ decisions about where to live, which could be affected by caregiving responsibilities for the surviving parent. Furthermore, we show that the decline in the number of children is not perfectly robust, as some of our robustness analyses do not show a statistically significant effect. Based on all this evidence, we conclude that parental death has little to no statistically significant effect on the fertility of the daughters.
Other studies investigating the impact of parental death on children’s fertility have produced mixed results. Apart from differences in institutional settings among the studied countries, we believe the differences in implemented empirical strategies to be particularly important. Existing studies are mainly correlational, using survival analysis, individual fixed effects, or simple linear regressions, comparing children who do and do not lose a parent. However, fertility trends before death differ between these two groups in our setting (see Fig. 1). We implement a credible causal identification strategy based on the timing of deaths, using only daughters who ultimately lose a parent during reproductive age. Compared to the majority of existing studies, our approach is designed to result in greater similarity in terms of (un)observed characteristics and expectations about parental death between treatment and control groups.Footnote 27 On top of this, we provide a series of robustness checks, including alternative control groups. We are confident that our results have an advantage in terms of credibility compared to previous studies.
Fertility rates have declined below replacement rates in many developed economies (Panel a of Fig. A.1). This development is likely to pose significant financial challenges for welfare systems in the future. Hence, designing appropriate policy measures to promote fertility is vital from an economic perspective. Our findings demonstrate that the decision to have children is not really affected by the death of parents. Therefore, focusing on intergenerational family aspects as a policymaker may not be the best choice to promote fertility. Other policies, like expanding childcare or financial incentives, might be more appropriate in this context (Hart et al. 2023).
The patterns identified in this study appear to be most relevant for modern, post-demographic transition societies, where fertility rates are generally lower, and family planning decisions are influenced by a variety of economic, cultural, and social factors. In such contexts, the resilience of fertility to external shocks, such as parental death, reflects the diminished direct impact of life expectancy on fertility decisions. In contrast, during the demographic transition, when mortality rates were higher and fertility was more closely tied to life expectancy, the loss of a parent might have had more profound implications for reproductive behavior. Thus, while our findings provide valuable insights into contemporary fertility dynamics, they are less likely to shed light on historical periods where the interplay between life expectancy and fertility was more pronounced (Galor 2011).
Data availability
The data are not publicly available.
Notes
There additionally exists a strain of the literature that looks at fertility responses to increases in mortality caused by natural disasters, wars, or other crises to investigate the macro-level relationship between mortality and fertility (see, e.g., Boberg-Fazlic et al. 2021; Caldwell 2004; Nandi et al. 2018; Nobles et al. 2015; Rodgers et al. 2005). These studies find that aggregate fertility goes up after an increase in aggregate mortality.
Utilizing one wave of US survey data, an undergraduate thesis suggests that parental death has a statistically insignificant effect on fertility (Chen 2020).
Persson and Rossin-Slater (2018) observe that women who experience the death of a relative during pregnancy are more likely to have additional children than mothers who experience the death shortly after giving birth. However, the authors consider a different research question. They do not focus on the effect of parental death per se but are mainly interested in the effects of in utero stress on child outcomes.
Jensen and Zhang (2023) use administrative data sources on various outcomes variables including fertility, labor market measures, and healthcare use; however, their main focus is on the labor market effect of parental death.
It has also been shown that daughters’ fertility decision impact their parents (e.g., Frimmel et al. 2022) and that parental divorce increases the likelihood of teenage pregnancy (e.g., Frimmel et al. forthcoming).
The Austrian Health Insurance Fund was preceded by nine provincial health insurance funds (Gebietskrankenkassen.). They were merged in 2020 to form this new entity.
Copayments include a prescription charge for medical drugs of 6.85 Euros (2020) and a small deductible for hospital stays.
Due to data limitations, we are not able to analyze the impact of the death of parents-in-law on women’s fertility. While, in principle, this analysis would strengthen the findings of our study, it has been shown that maternal grandparents tend to be more important than paternal grandparents for informal childcare (see, e.g., Thomese and Liefbroer 2013).
Upper Austria is one of the nine federal provinces of Austria. Its more than 1.5 million inhabitants account for 16.73 percent of Austria’s population (see Statistics Austria).
Note that our sample includes all death causes. Information on death causes is only available until 2009.
Note that annual wages are top-coded due to the maximum assessment basis for social security contributions.
The process of assigning placebo death years involves three steps: First, all daughters born in the same year are kept. Second, the empirical distribution of death years among treated daughters is obtained. Finally, death years are randomly assigned to daughters without parental death, ensuring that the distribution of placebo death years matches the distribution of actual death years. This process is performed for all birth years of treated daughters in the sample.
We want to analyze parental deaths during reproductive age. Therefore, we restrict the treatment group to daughters who experience the actual death of their parents between the ages of 25 and 39. We restrict the control daughters to be in the same age range (25 to 39) at the time of the comparison with the treatment group in the year d. Since we set \(\tau \) to 5, it follows that control daughters are between 30 and 44 at the time of their actual parental death and between 25 and 39 at the time of their placebo parental death. Furthermore, since we analyze parental deaths between 2000 and 2018 and set \(\tau \) to 5, treated daughters experience their actual death between 2000 and 2013 and control daughters between 2005 and 2018.
Note that we deviate from the original methodology in Fadlon and Nielsen (2019) in two ways. First, they focus on health shocks as a treatment, whereas we consider deaths. Second, Fadlon and Nielsen (2019) include only sudden health shocks in their treatment definition, while in our main analysis, we use deaths due to all causes. To make our setting more comparable, we also analyze sudden deaths in a robustness check in Section 4.4.
Note that the earliest possible age when daughters in our treated group can experience a parental death is 25.
Each daughter in the control pool can be matched with multiple treated daughters. However, as Panel c of Fig. A.5 in the Supplementary Material shows, around 40 percent of daughters in the control pool are used only once as a match.
Note that there are two main differences between our approach and the matching procedure in Jensen and Zhang (2023). First, we match each treated daughter with 5 nearest neighbors, not just one. Second, we also include both daughter and parent characteristics, while Jensen and Zhang (2023) use only children’s characteristics. The list of covariates is also slightly different. For example, Jensen and Zhang (2023) include children’s education level, which is not available in our data.
We have defined binary indicators that are one if a daughter has a birth of the respective order in a given year. The binary indicators are zero, if either no birth was recorded in a given year or a birth was recorded, but it was not of the respective birth order.
To measure the supply of formal childcare, we use the number of groups in formal childcare facilities (nurseries, kindergarten, and after-school care centers) per 1000 inhabitants of a postal code area. The raw data were obtained from Statistics Austria and are available between 2005 and 2019. We convert the data from municipal to postal code level using the weights provided by Pennerstorfer (2021).
An alternative hypothesis about the availability of siblings and the loss of informal childcare capacities is that the loss of informal childcare is larger if a woman has siblings, as this would imply that the surviving parent potentially has to look after the grandchildren of multiple families. If a woman has no siblings, the surviving parent can direct all their childcare capacities toward one set of grandchildren.
To calculate the driving duration, we retrieve the postal codes of the daughter and surviving parent. We then use the R-package opencage to geocode the postal codes and obtain their coordinates. Finally, we utilize the R-package osrm to determine the driving duration in minutes between the postal code centroids.
Note that the driving duration can only be computed if both the daughter and the surviving parent reside in Upper Austria. The maximum driving duration is limited due to the small size of Upper Austria. This is evident from the average driving duration of only 14.80 min between daughters and surviving parents in the period preceding the parental death.
Care allowance is a lump-sum benefit paid by the government to help cover some of the costs of care. It is paid on application and the exact amount depends on the level of care required (see oesterreich.gv.at, available in German only).
Note that we find a larger reduction in the number of children using our matched control group than Jensen and Zhang (2023). However, the results are not directly comparable due to differences in the matching procedure.
In our main analysis sample, 13,886 women are only in the treatment group, 22,980 women are only in the control group, and 13,420 women are in both groups. The overlap is therefore around 27 percent.
Our results are also comparable to the findings of Jensen and Zhang (2023), who also use a causal identification strategy. They find that parental death reduces the total number of children by 0.003 to 0.012, which is in line with our finding that the cumulative number of children decreases by a quantitatively insignificant amount of no more than 0.0086 after the death of a parent.
References
Ahammer A, Wiesinger R, Zocher K (2021) The Austrian healthcare system: changes and challenges. In: Baltagi BH, Moscone F (eds) The sustainability of healthcare systems in Europe. Contributions to Economic Analysis Vol. 295, Emerald Publishing Limited, Bingley, UK, pp 153–166
Ahammer A, Glogowsky U, Halla M, Hener T (2023) The parenthood penalty in mental health: evidence from Austria and Denmark. Working Paper No. 2312. Department of Economics, Johannes Kepler University, Linz
Angelov N, Johansson P, Lindahl E (2016) Parenthood and the gender gap in pay. J Labor Econ 34(3):545–579
Aparicio-Fenoll A, Vidal-Fernandez M (2015) Working women and fertility: the role of grandmothers’ labor force participation’. CESifo Econ Stud 61(1):123–147
Appel CW, Johansen C, Christensen J, Frederiksen K, Hjalgrim H, Dalton SO, Dencker A, Dige J, Bøge P, Dyregrov A, Mikkelsen OA, Lund LW, Høybye MT, Bidstrup PE (2016) Risk of use of antidepressants among children and young adults exposed to the death of a parent. Epidemiology 27(4):578–585
Battistin E, Nadai MD, Padula M (2014) Roadblocks on the road to grandma’s house: fertility consequences of delayed retirement IZA Discussion Paper No. 8071, Institute for the Study of Labor, Bonn
Beaujouan É, Solaz A (2023) Polarized adult fertility patterns following early parental death. Popul Stud 77(2):217–239
Berg L, Rostila M, Arat A, Hjern A (2019) Parental death during childhood and violent crime in late adolescence to early adulthood: a Swedish national cohort study. Palgrave Commun 5(74):1–8
Boberg-Fazlic N, Ivets M, Karlsson M, Nilsson T (2021) Disease and fertility: evidence from the 1918–19 influenza pandemic in Sweden. Econ Hum Biol 43:1–27
Böckerman P, Haapanen M, Jepsen C (2023) Dark passage. Mental health consequences of parental death. Am J Health Econ 9(4):584–604
Bozzoli CG (2016) Orphanhood and fertility in young adults: evidence from South Africa. Econ Hum Biol 22:190–200
Caldwell JC (2004) Social upheaval and fertility decline. J Fam Hist 29(4):382–406
Chen J (2020) Estimating the effect of grandparent death on fertility. Undergratduate Honors Thesis, Berkeley Economics. University of Carlifornia, Berkeley, CA
Dahlberg J (2020) Death is not the end: a register-based study of the effect of parental death on adult children’s childbearing behavior in Sweden. OMEGA-J Death Dying 81(1):80–106
Del Boca D (2002) The effect of child care and part time opportunities on participation and fertility decisions in Italy. J Popul Econ 15:549–573
Eibich P, Siedler T (2020) Retirement, intergenerational time transfers, and fertility. Eur Econ Rev 124:103392
Fadlon I, Nielsen TH (2019) Family health behaviors. Am Econ Rev 109(9):3162–3191
Fadlon I, Nielsen TH (2021) Family labor supply responses to severe health shocks: evidence from Danish administrative records. Am Econ J Appl Econ 13(3):1–30
Frimmel W, Halla M, Schmidpeter B, Winter-Ebmer R (2022) Grandmothers’ labor supply. J Hum Resour 57(5):1645–1689
Frimmel W, Halla M, Paetzold J, Schmieder J (forthcoming) Health of parents, their children’s labor supply, and the role of migrant care workers. J Labor Econ
Frimmel W, Halla M, Winter-Ebmer R (forthcoming) How does parental divorce affect children’s long-term outcomes? J Public Econ
Galor O (2011) Unified growth theory. Princeton University Press
Galor O (2022) The journey of humanity: the origins of wealth and inequality. Penguin
Glaser F, Pruckner GJ (2023) A hard pill to swallow? Parental health shocks and children’s mental health. Health Econ 32(12):2768–2800
Hank K, Buber I (2009) Grandparents caring for their grandchildren: findings from the 2004 survey of health, ageing, and retirement in Europe. J Fam Issues 30(1):53–73
Hart R, Bergsvik J, Fauske A, Kim W (2023) Causal analysis of policy effects on fertility. CESifo Working Paper No. 10690, CESifo, Munich
Hiyoshi A, Berg L, Grotta A, Almquist Y, Rostila M (2021) Parental death in childhood and pathways to increased mortality across the life course in Stockholm, Sweden: a cohort study. PLoS Med 18(3):e1003549
Ilciukas J (2023) Fertility and parental retirement. J Public Econ 226:104928
Jensen MF, Zhang N (2023) Effects of parental death on labor market outcomes and gender inequalities. Discussion Paper No. 1018, Department of Economics, University of Oxford, Oxford
Kailaheimo-Lönnqvist S, Erola J (2020) Child’s age at parental death and university education. Eur Soc 22(4):1–23
Kailaheimo-Lönnqvist S, Kotimäki S (2020) Cause of parental death and child’s health and education: the role of parental resources. SSM Popul Health 11:1–17
Kaindl M, Wernhart G (2012) Wie Großeltern ihre Kinder und Enkelkinder unterstützen: persönliche und finanzielle Hilfe von Großeltern aus Sicht der Großeltern und der erwachsenen Kinder, Vol. 78 of Working Paper / Österreichisches Institut für Familienforschung, Österreichisches Institut für Familienforschung an der Universität Wien, Wien
Kertzer DI, White MJ, Bernardi L, Gabrielli G (2009) Italy’s path to very low fertility: the adequacy of economic and second demographic transition theories. Eur J Popul 25:89–115
Kidman R, Anglewicz P (2014) Fertility among orphans in rural Malawi: challenging common assumptions about risk and mechanisms. Int Perspect Sex Reprod Health 40(4):164–175
Kleven H, Landais C, Søgaard JE (2019) Children and gender inequality: evidence from Denmark. Am Econ J Appl Econ 11(4):181–209
Kristiansen IL (2021) Consequences of serious parental health events on child mental health and educational outcomes. Health Econ 30(8):1772–1817
Leopold T, Lechner CM (2015) Parents’ death and adult well-being: gender, age, and adaption to filial bereavement. J Marriage Fam 77(3):747–760
Marcos MAT (2023) Grandmothers and the gender gap in the Mexican labor market. J Dev Econ 162:103013
Marks NF, Jun H, Song J (2007) Death of parents and adult psychological and physical well-being. J Fam Issues 28(12):1611–1638
Nandi A, Mazumdar S, Behrman JR (2018) The effect of natural disaster on fertility, birth spacing, and child sex ratio: evidence from a major earthquake in India. J Popul Econ 31:267–293
Nobles J, Frankenberg E, Thomas D (2015) The effects of mortality on fertility: population dynamics after a natural disaster. Demography 52(1):15–38
Norén A (2020) Sick of my parents? Consequences of parental ill health on adult children. Working Paper No. 2020:1, Institute for Evaluation of Labour Market and Education Policy (IFAU), Uppsala
Okun BS, Stecklov G (2021) The impact of grandparental death on the fertility of adult children. Demography 58(3):847–870
Pennerstorfer D (2021) Converting variables between non-hierarchical regions: the case of austrian municipalities and ZIP-Code Areas. Working Paper No. 2111. Department of Economics, Johannes Kepler University, Linz
Persson P, Rossin-Slater M (2018) Family ruptures, stress, and the mental health of the next generation. Am Econ Rev 108(4–5):1214–1252
Pessin L, Rutigliano R, Potter MH (2022) Time, money, and entry into parenthood: the role of (grand)parental support. J Marriage Fam 84(1):101–120
Pink S (2018) Anticipated (grand-)parental childcare support and the decision to become a parent. Eur J Popul 34(5):691–720
Rackin HM, Gibson-Davis CM (2022) Familial deaths and first birth. Popul Dev Rev 48(4):1027–1059
Rellstab S, Bakx P, García-Gómez P, van Doorslaer E (2020) The kids are alright - labour market effects of unexpected parental hospitalisations in the Netherlands. J Health Econ 69:102275
Reneflot A (2011) Childhood family structure and reproductive behaviour in early adulthood in Norway. Eur Sociol Rev 27(1):56–69
Rodgers JL, St. John CA, Coleman R (2005) Did fertility go up after the Oklahoma City bombing? An analysis of births in metropolitan counties in Oklahoma, 1990–1999. Demography 42(4):675–692
Rostila M, Saarela JM (2011) Time does not heal all wounds: mortality following the death of a parent. J Marriage Fam 73(1):236–249
Rutigliano R (2020) Counting on potential grandparents? Adult children’s entry into parenthood across European countries. Demography 57(4):1393–1414
Rutigliano R (2023) Do grandparents really matter? The effect of regular grandparental childcare on the second-birth transition. Eur Sociol Rev 1–14
Thomese F, Liefbroer AC (2013) Child care and child births: the role of grandparents in the Netherlands. J Marriage Fam 75(2):403–421
Wilcox HC, Kuramoto SJ, Lichtenstein P, Långström N, Brent DA, Runeson B (2010) Psychiatric morbidity, violent crime, and suicide among children and adolescents exposed to parental death. J Am Acad Child Adolesc Psychiatry 49(5):514–523
Zweimüller J, Winter-Ebmer R, Lalive R, Kuhn A, Wuellrich JP, Ruf O, Büchi S (2009) Austrian social security database. Working Paper No. 0903, The Austrian Center for Laobr Economics and the Analysis of the Welfare State, Johannes Kepler University, Linz
Acknowledgements
We would like to thank editor Oded Galor and four anonymous referees. Their suggestions and insights improved this paper significantly. For helpful discussions and comments, we thank Gerald J. Pruckner, Wolfgang Frimmel, Analisa Packham, Lindsey Rose Bullinger, David Bradford, Rudolf Winter-Ebmer, Katrin Zocher, and participants at ESPE 2023, EEA 2023, VfS Annual Conference 2023, NOeG 2023, JKU Economics Lunch Time Seminar 2023, Vienna Economics PhD Workshop 2023, and PhD Seminar at the University of Innsbruck 2024.
Funding
Open access funding provided by Johannes Kepler University Linz. Financial support from Heinrich Graf Hardegg’sche Stiftung is gratefully acknowledged.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Responsible editor: Oded Galor.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Glaser, F., Wiesinger, R. Life after loss: the causal effect of parental death on daughters’ fertility. J Popul Econ 38, 6 (2025). https://doi.org/10.1007/s00148-025-01057-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00148-025-01057-8