
Abstract
Purpose
Estimates of parenthood in individuals with psychosis range from 27 to 63%. This number has likely increased due to the introduction of newer anti-psychotics and shorter hospital stays. The problems of psychosis can affect patients’ capacity to offer the consistent, responsive care required for healthy child development. The following research questions were assessed: (1) what proportion of these patients have their children correctly recorded in their clinical notes, (2) what proportion of patients in secondary care with a psychotic diagnosis have children, and (3) what sociodemographic characteristics are associated with parenthood in this population.
Methods
This study used CRIS (Clinical Record Interactive Search) to search for patients with a diagnosis of non-affective or affective psychosis (F20–29, F31.2 or F31.5) within a UK NHS Trust. A binomial regression model was fitted to identify the variables associated with parenthood.
Results
Fewer than half of the parents in the sample had their children recorded in the correct field in their clinical notes. Of 5173 patients with psychosis, 2006 (38.8%) were parents. Characteristics associated with parenthood included being female, older age, higher socioeconomic status, renting or owning, having ever been married, being unemployed, not being White (British) and not having a diagnosis of schizophrenia.
Conclusion
Over one-third of patients with psychosis were parents, and the study indicates that not all NHS Trusts are recording dependants accurately. Many variables were strongly associated with parenthood and these findings may help target interventions for this population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The positive and negative symptoms of psychosis and side effects from antipsychotic medication can affect a parent’s capacity to look after their child [1]. Furthermore, the children of parents with psychosis are more likely than the children of parents without a mental health diagnosis to have behavioural and psychological difficulties [2] and are at an increased likelihood of taking on a caring role for their parents or siblings [3].
Recording of children on patients’ clinical records
Parents with psychosis are often reluctant to seek help due to fear of being criticised as a parent or the possibility of social services involvement [4]. As a result of this, and of service providers being hesitant to ask about their children, dependants are often not present in their parents’ clinical records, making them invisible to services [5]. Policies in Norway [6], Sweden [7] and Australia [8] now require that adult mental health services record the presence of children accurately and work to meet the needs of the whole family. In the UK, the ‘Think Family’ initiative [9] called for improvement in the identification of patients’ children to signpost these families to relevant services and to safeguard the children as necessary.
Global estimates of parental psychosis and factors associated with parenthood
An accurate estimate of how many people with psychosis are parents, and what characteristics are associated with parenthood, is needed to inform interventions for these families. The most recent estimates of parenting amongst people with psychosis have been conducted in Australia [10] and Germany [11], which were 27% and 38%, respectively. The most recent study in the UK was conducted over 20 years ago and reported that 63% of the 246 women with psychosis in a secondary care sample were mothers [12]. More recent estimates of the number of parents in UK adult mental health services have looked at any mental health diagnosis e.g. [13, 14], rather than psychosis specifically. The current rate is likely to be different since newer anti-psychotics and shorter hospital stays have increased fertility and opportunity to have children, respectively [15, 16].
It is also necessary to investigate factors that are associated with parenting status within those with a psychotic diagnosis. Certain characteristics have previously been shown to be associated with a better quality of care from parents with psychosis. For example, social class and lone parenthood [17] as well as illness severity [18]. By ascertaining which factors are associated with parenthood alongside the knowledge of which factors are associated with quality of care in parents, this will provide more information on the needs of parents with psychosis and inform more targeted interventions. Factors such as gender, age, marital status, and accommodation have previously been shown to be associated with parenting status [12, 19, 20]. This study will investigate these characteristics in a UK sample as well as others where there is mixed evidence for their association including diagnosis, ethnicity, and employment [12, 19, 20].
This study used CRIS, the Clinical Record Interactive Search, to estimate the proportion of patients with psychosis in an NHS Trust who have a child, to examine the recording of child details in UK electronic health records, and to understand some of the characteristics of these families.
Research questions
-
1.
What proportion of children are recorded in the correct structured field of their parents’ clinical notes?
-
2.
What proportion of patients within an NHS Trust with a psychotic diagnosis have a child?
-
3.
What are the sociodemographic factors that characterise being a parent with a psychotic diagnosis?
Methods
This is a cross-sectional study using de-identified patient records from a UK mental health service case register.
CRIS (clinical records interactive search)
CRIS is a database that contains over 2 million de-identified patient records from 14 NHS trusts across the UK, and allows the analysis of both structured and free-text data in an individual’s clinical records [21, 22]. This study accessed data from one of these Trusts.
Study cohort
The CRIS system was searched on February 14th 2019 for all patients who had at any time been given an ICD 10 diagnosis of psychosis (F20–29, F31.2 or F31.5) or whose assigned cluster level indicated the presence of psychotic symptoms (cluster levels 10–14 and 16–17), yielding 5764 participants. To produce an estimate of parenthood at one point in time, those who had died on or before February 14th 2019 were removed from the sample, giving a final sample of 5173 participants.
Study outcome
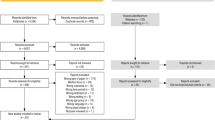
The primary outcome in this study was parent status (1 = participant is a parent; 0 = participant is not a parent). The sample was searched to see if any child details had been entered in the patient’s ‘contacts’ field, where the relationship was listed as ‘son’, ‘daughter’, ‘dependant’ or ‘stepchild’ (see Fig. 1). Children were defined as biological children or step-children of any age and it was not a requirement for them to be currently living with or cared for by the parent. The primary researcher then collected the free-text clinical notes of the patients who did not have children recorded in their ‘contacts’ field to determine whether any of these patients had children mentioned in their free-text clinical notes.

Identifying children in clinical notes
To gain an accurate estimate of how many patients in the sample had children, searches were then conducted in patients’ free-text clinical notes to identify any further children. A pilot search of ‘son’, ‘daughter’ and ‘child’ returned many irrelevant notes, and therefore, it was decided to search the notes for ‘no children’ first, to identify non-parents, and then search the remaining notes for ‘son’ or ‘daughter’.
For searches in the free-text clinical notes, the following process was followed (see also Fig. 1):
-
1.
An initial search of free-text notes was conducted for the phrase ‘no children’ amongst the participants who did not have any children recorded in the ‘contacts’ field.
-
2.
The notes returned from this search were read to confirm this did indeed mean that these participants did not have children or if ‘no children’ was referring to something other than the patient’s parenthood. These notes were also searched for the words ‘son’ or ‘daughter’ to check if the patient had not later become a parent before February 14th 2019.
-
3.
A second search of free-text notes was conducted for any instances of the words ‘son’ or ‘daughter’ amongst those participants who did not have any children recorded in the ‘contacts’ field and did not have any notes returned from the initial search of free-text notes.
-
4.
Each of these clinical notes was read to confirm the presence of children and extract data on the number, ages and genders of children, where it was reported.
-
5.
The participants who did not have any clinical notes returned from these two searches were checked to see if their clinical notes were indeed populated, where the presence of a child might have been recorded. Once this was confirmed, these participants were assumed not to have any children.
Independent variables
The following variables were extracted from the structured fields of all participants: gender, date of birth, ethnicity, marital status, employment, accommodation, LSOA (Lower Layer Super Output Area) marker, smoking status, ward stays and diagnosis.
Date of birth was used to derive participants’ ages on February 14th 2019. Ethnicity, marital status, employment, accommodation, smoking status and diagnosis were collapsed into broader categories to avoid small cell counts. LSOAs are geographic areas in the UK with an average population size of 1500, which can be linked to postcodes. Each LSOA marker was combined with the Office for National Statistics Index of Multiple Deprivation (IMD) [23] allowing each participant to be ranked against others living in different LSOAs in terms of deprivation. The IMD is based on 39 separate indicators across the seven domains of income, employment, education, health, crime, barriers to housing and services, and living environment, and is the official measure of relative deprivation in England [23]. These rankings were separated into nine equally sized groups of decreasing deprivation levels.
If multiple entries had been recorded for a participant on any variable, the most recent entry was selected to be used in the analysis.
Analysis
To examine the sociodemographic differences between parents and non-parents, the relationship between parent status and each independent variable was tested individually using a t-test if the variable was continuous or ordinal, or a Chi-squared test if the variable was discrete or categorical. Those with missing data for the variable in question were first included and then excluded to determine whether it was the missingness that was significant between the two groups.
A binomial regression model was then fitted to determine which variables were most associated with whether a participant was a parent or not. There was a large amount of missing data for some variables, and due to nature of administrative data, it was assumed that this missingness was not at random (MNAR), whereby the missingness of a variable is related to the variable itself. Missing values for each variable were grouped into an additional category (labelled ‘unknown’) for the analysis. Although the missing indicator method is not usually recommended since it can introduce bias, it has been shown to be a good option when data are MNAR compared to methods such as multiple imputation or listwise deletion [24].
As a sensitivity analysis, the modelling was refit on a subset of the study cohort that excluded any participants without dependants (i.e. all children were 18 and over). This compared parents with dependant children and non-parents. All statistical analyses were performed in R (v4.0.2).
Results
Accuracy of recording of patients’ children in their clinical notes
Among the study cohort (n = 5173), 824 had children recorded in the structured field ‘contacts’ (Fig. 1). After searching the remaining 4349 for the phrase ‘no children’ in their free-text clinical notes, 629 records were returned and after reading these notes, 574 were confirmed not to have any children. The free-text search ‘son’ or ‘daughter’ returned 2548 participants’ clinical notes and, after reading these, a further 1182 showed evidence of having a child.
Proportion of parents in the sample
In total, 2006 (38.8%) out of 5173 patients with psychosis were reported to have children. The remaining 3167 (61.2%) were assumed not to have children after extensive searching (Fig. 1).
Demographic details of children
The 2006 parents in the sample had 3745 children in total. The mean average number of children was 1.87 per parent and the median value was 2. Most parent participants did not have any dependant children (see Supplementary table 1). Over two-thirds (67.2%) of parents with a least one dependant had their child’s details recorded correctly in the ‘contacts’ field of their notes, and just over a half (54.9%) of parents of non-dependants had them recorded in the ‘contacts’ field. The demographic details of the children are presented in Supplementary table 2. Some of these details were available from the CRIS data; however, the majority of them were obtained through reading patients’ clinical notes. Although it was often clear whether the child was under or over the age of 18, it was less likely that the exact age of the child would be acquired through reading the notes.
Demographic details of participants
Table 1 shows the sociodemographic characteristics of parents and non-parents in the sample.
The two groups were significantly different in terms of age (t(4178.5) = − 29.6, p < 0.001), gender (X2(2, N = 5173) = 394.05, p < 0.001), ethnicity (X2(6, N = 5173) = 17.76, p = 0.007), marital status (X2(3, N = 5173) = 1162.9, p < 0.001), accommodation (X2(4, N = 5173) = 188.41, p < 0.001), employment (X2(5, N = 5173) = 261.06, p < 0.001), and diagnosis (X2(8, N = 5173) = 102.87, p < 0.001), both when including and excluding those with missing data. In terms of directionality, parents were older than non-parents, and a higher proportion of parents were female, married or divorced, retired or unemployed, owning or renting. A lower proportion of parents had a diagnosis of schizophrenia and were White (British).
The number of ward stays was originally non-significant (t(4495.8) = − 0.168, p = 0.8667) but became significant when excluding those who did not have a ward stay recorded (t(2552.7) = 1.988, p = 0.0458). The mean average number of ward stays between parents and non-parents was almost identical (1.89 for parents and 1.88 for non-parents); however, when excluding those without any ward stay recorded, the average ward stays of parents rises to 3.41 and non-parents to 3.71. IMD was not significant (t(4231.1) = − 0.650, p = 0.5155) and smoking status was initially significant (X2(3, N = 5173) = 10.73, p = 0.013) but became non-significant when those with missing data were excluded (X2(2, N = 2454) = 3.88, p = 0.144).
Regression modelling
All ten participant-level variables (age, gender, ethnicity, marital status, accommodation, employment, diagnosis, ward stay, smoking and index of multiple deprivation) were included in the model. Table 2 presents the mutually adjusted odds ratio of being a parent for each variable in the model.
A higher age and number of ward stays were both positively associated with parenthood. Participants living in less deprived neighbourhoods were slightly less likely to be a parent. Women in the sample were more than twice as likely to be parents as men in the sample. Patients who were married or divorced were more likely to have a child when compared with participants who were single. When compared to participants who were White—British, most other ethnicities had higher odds of being a parent. For accommodation, participants who were owning or renting were twice as likely as those in supported living to be a parent. Participants who were recorded as unemployed were more likely to be a parent than those who were students, retired or in employment, with students being the least likely group to have children. Participants with non-schizophrenia psychoses were also more likely to have children than participants with a diagnosis of schizophrenia. Current smokers were more likely to be parents than non-smokers.
The sensitivity analysis, i.e. parents with dependant children and non-parent participants, produced similar findings (see Supplementary table 3).
Discussion
Recording of patients’ children
The first aim of this study was to establish whether children are recorded in the correct place on patients’ clinical notes. Out of the 2006 parents that were identified, fewer than half of them had their children recorded in the appropriate structured field. Instead, the majority were identified by searching free-text notes and then reading through each note to confirm the presence or absence of a child. Even for the patients who had children entered in the appropriate field, the dates of birth of these children were often not recorded. Although dependants were more likely to be recorded than non-dependants, these findings nevertheless suggest that further work with staff is needed to meet the requirements for recording children accurately in this Trust [9].
The proportion of those with a diagnosis of psychosis who are a parent
Over a third (38.8%) of the 5173 patients with psychosis were parents. More than half (53.9%) of female patients with psychosis were mothers and around a quarter (26.9%) of male patients with psychosis were fathers. The rate found in this study is very similar to the most recent international estimate conducted by a national survey in Australia, which found that 38.1% of the 1825 participants were parents, with 56.2% of women being mothers and 25.9% of men being fathers [10]. Due to increasingly shorter hospital stays and the usage of newer anti-psychotics within women with psychosis [15, 16], we expected that the result of this study would be higher than the estimate from a previous study conducted in the UK, which reported that 63% of women with psychosis were mothers [12]. The reasons for our lower estimate are currently unclear. We know that Howard et al. [12] made attempts to establish epidemiological representative cases, although the smaller sample size of 246 may have resulted in an overestimate of the true proportion. Recently, it has been shown that women with a psychotic diagnosis in a UK sample have a lower fertility rate than the general population [25]; however, this does not account for women who develop psychosis after becoming a mother. Indeed, another recent study in the US found similar rates of parenthood in a sample with serious mental illness compared to a sample without a mental health diagnosis [26].
Factors associated with parenthood
An examination of the factors associated with parenthood found significant differences between parents and non-parents in age, gender, ethnicity, marital status, diagnosis, employment and accommodation. Older age, a higher number of ward stays, higher socioeconomic status, being female, renting or owning their home, having ever been married, not having schizophrenia, being unemployed, not being White British and being a current smoker were all important factors associated with parenthood. Many of these variables, such as being older or renting/owning a home, point towards a more settled lifestyle, possibly, giving individuals with psychosis more opportunities to meet a partner and have children.
The results from this model identified that women with psychosis were much more likely than men to be a parent. Other studies have also confirmed gender as an important variable in whether one has a child with a psychotic diagnosis [10, 12, 20]. More parents with psychosis have their first psychotic episode after becoming a parent rather than before [12, 18, 27]. Since psychosis has an earlier age of onset in men than in women, elements related to psychosis such as poverty and isolation [28] may provide men with fewer opportunities to have children. It might also be the case that the true incidence of parenthood within men with psychosis is under-reported. Since parenthood was recorded whenever there was a mention of children, and men with psychosis are less likely to have contact with their children [29], the parenting status of some men in this sample may have been missed.
Those with a diagnosis of acute psychotic disorder (F23) were much more likely than those diagnosed with schizophrenia (F20) to have children and those with bipolar disorder with psychotic symptoms (F31.2 or F31.5) were also more likely. Schrank et al. [20] also found that those with a diagnosis of schizophrenia were the least likely to have children when compared to other psychotic diagnoses. To be diagnosed with schizophrenia, both positive and negative symptoms must be present. Individuals with schizophrenia are also more likely than those with another psychotic disorder to experience cognitive symptoms and for these symptoms to be chronic rather than episodic [30]. The differences between these diagnoses in this study might reflect the fact that a higher symptom severity can lead to fewer opportunities to meet a partner and have children.
The missing indicator method was used to address the missing data in the regression analysis. It is not possible to prove whether data are missing at random (MAR) or missing not at random (MNAR) without follow-up of participants, which due to the design of this study is not possible. However, there is strong reason to hypothesise that the data were MNAR, and thus the missing indicator method was appropriate, due to the nature of administrative data. For example, there were high levels of missing data for smoking status. It is well known that smoking status is more likely to be missing for non-smokers than smokers in health records [31]. This study had 23% of participants recorded as smokers. In the UK, around 37% of those with a mental health condition are smokers [32], meaning the large amount of missing data in this variable (47%) is likely to be mostly attributable to non-smokers rather than smokers. Therefore, it seems likely that non-smokers were less likely to have their smoking status recorded and that the missingness within the smoking status variable was attributable to smoking status itself.
Strengths and limitations
A strength of this study is that it updated the estimate of the proportion of patients with psychosis who are parents in the UK, based on data from an NHS Trust sample. Extensive work was done to identify children by reading the clinical notes of patients. However, due to the time it took to identify parent status in this study’s cohort, it was not possible to perform an analysis whereby this cohort of parents with a psychotic diagnosis was matched with another cohort of parents (e.g. parents with a diagnosis of depression), to examine whether the sociodemographic factors identified are specific to psychosis.
Using administrative data meant the study was limited to the information completed by healthcare professionals. This resulted in a large amount of missing data, especially in relation to employment, accommodation and smoking status. Including more factors about the child, such as contact with child and family services, accessing child mental health services, and education level, may have informed this analysis, but these variables are not available when using the CRIS dataset.
Due to the data likely being MNAR, and the outcome in this study (parenthood) being common, the estimates obtained may be biased, and therefore, should be interpreted with caution with focus on the directionality rather than specific estimates obtained. The aim of this study was to identify characteristics amongst patients with psychosis that are associated with parenthood, and therefore, another limitation is that no conclusions can be drawn about the temporal relationships between each independent variable and parenthood.
Implications for practice and research
Although the Think Family initiative [9] recommends the recording of children on patients’ clinical notes, the current findings suggest that this may still not be happening systematically and comprehensively. Children of parents with psychotic disorders are at risk of emotional and behavioural difficulties during childhood [33] and psychopathology later in life [34]. Interventions currently exist to provide support to these children by explaining their parent’s illness [35], linking the family with a caseworker [36], and providing treatment for children’s own mental health difficulties [37]. However, before receiving support, these children must be accurately identified, and that information should also be shared between adult mental health services and other agencies [38]. We can see from global examples that it is possible to increase the identification of these children. For example, after changes to legislation and the introduction of the ‘Assessment Form’ in Norway, rates of identification of patients’ parenting status increased [6].
This study has established that within the UK, over a third of patients with a psychotic diagnosis will also be a parent. Healthcare professionals working with these patients would likely benefit from training in providing family-focussed care which may include recognising the centrality of patients’ parenting role, providing age-appropriate information to children, creating a family-friendly environment during inpatient visits and referring families to additional supports [39]. This study also highlighted that some patients with psychosis are more likely to be parents than others, including those who are female and of an older age. This information will help healthcare professionals in targeting interventions and support to certain client groups.
CRIS provides large datasets representing an anonymised form of a patient’s clinical notes. Future research on parents with psychosis and their children could benefit from using additional CRIS datasets from more than one Trust and enabling natural language processing to improve the identification of children in patients’ notes. The CRIS dataset could also be linked with other datasets to obtain more details on the parents and their children; for example, with the Hospital Episode Statistics (HES) database [40], which would allow all children born to the parent to be identified.
Availability of data and materials
Data are not publicly available and can only be accessed using CRIS, which provides access to anonymised data from patients’ clinical records. For more information, please contact the CRIS Administrator at CRIS.Admin@oxfordhealth.nhs.uk.
Code availability
The R code used in this analysis is available here https://github.com/JessRadley/CRIS-parents-with-psychosis.
References
Campbell LE, Poon AWC (2020) Parenting challenges for persons with a serious mental illness. Ment Heal Soc Work. https://doi.org/10.1007/978-981-13-6975-9
Dean K, Stevens H, Mortensen PB, Murray RM, Walsh E, Pedersen CB (2010) Full spectrum of psychiatric outcomes among offspring with parental history of mental disorder. Arch Gen Psychiatry 67:822–829
Ackerson B (2003) Coping with the dual demands of severe mental illness and parenting: the parents’ perspective. Fam Soc J Contemp Soc Serv 84:109–118. https://doi.org/10.1606/1044-3894.69
Blegen NE, Hummelvoll JK, Severinsson E (2010) Mothers with mental health problems: a systematic review. Nurs Health Sci 12:519–528. https://doi.org/10.1111/j.1442-2018.2010.00550.x
Maybery DJ, Reupert AE (2009) Parental mental illness: a review of barriers and issues for working with families and children. J Psychiatr Ment Health Nurs 16:784–791. https://doi.org/10.1111/j.1365-2850.2009.01456.x
Lauritzen C, Reedtz C, Rognmo K, Nilsen MA, Walstad A (2018) Identification of and support for children of mentally ill parents: a 5 year follow-up study of adult mental health services. Front Psychiatry 9:1–10. https://doi.org/10.3389/fpsyt.2018.00507
Afzelius M, Östman M, Råstam M, Priebe G (2018) Parents in adult psychiatric care and their children: a call for more interagency collaboration with social services and child and adolescent psychiatry. Nord J Psychiatry 72:31–38. https://doi.org/10.1080/08039488.2017.1377287
Goodyear M, Maybery DJ, Reupert AE, Allchin B, Fraser C, Fernbacher S et al (2017) Thinking families: a study of the characteristics of the workforce that delivers family-focussed practice. Int J Ment Health Nurs. https://doi.org/10.1111/inm.12293
Diggins M. Think child, think parent, think family: A guide to parental mental health and child welfare. 2011.
Campbell LE, Hanlon MC, Poon AWC, Paolini S, Stone M, Galletly C et al (2012) The experiences of Australian parents with psychosis: The second Australian national survey of psychosis. Aust N Z J Psychiatry 46:890–900. https://doi.org/10.1177/0004867412455108
Jungbauer J, Kuhn J, Lenz A (2011) On prevalence of parenthood in schizophrenia patients. Gesundheitswesen 73:286–289. https://doi.org/10.1055/s-0030-1252038
Howard LM, Kumar R, Thornicroft G (2001) Psychosocial characteristics and needs of mothers with psychotic disorders. Br J Psychiatry 178:427–432. https://doi.org/10.1192/bjp.178.5.427
Ruud T, Maybery DJ, Reupert AE, Weimand B, Foster K, Grant A et al (2019) Adult mental health outpatients who have minor children: prevalence of parents, referrals of their children, and patient characteristics. Front Psychiatry 10:1–14. https://doi.org/10.3389/fpsyt.2019.00163
Gatsou L, Yates S, Hussain S, Barrett M (2016) Parental mental illness: incidence, assessment and practice. Ment Heal Pract 19:25–27
Vigod SN, Seeman MV, Ray JG, Anderson GM, Dennis CL, Grigoriadis S et al (2012) Temporal trends in general and age-specific fertility rates among women with schizophrenia (1996–2009): A population-based study in Ontario. Canada Schizophr Res 139:169–175. https://doi.org/10.1016/j.schres.2012.05.010
Seeman MV (2009) The changing role of mother of the mentally ill: from schizophrenogenic mother to multigenerational caregiver. Psychiatry 72:284–294
Howard LM, Thornicroft G, Salmon M, Appleby L (2004) Predictors of parenting outcome in women with psychotic disorders discharged from mother and baby units. Acta Psychiatr Scand 110:347–355. https://doi.org/10.1111/j.1600-0447.2004.00375.x
Campbell LE, Hanlon MC, Galletly CA, Harvey C, Stain H, Cohen M et al (2018) Severity of illness and adaptive functioning predict quality of care of children among parents with psychosis: a confirmatory factor analysis. Aust N Z J Psychiatry 52:435–445. https://doi.org/10.1177/0004867417731526
Hearle J, Plant K, Jenner L, Barkla J, McGrath J (1999) A survey of contact with offspring and assistance with child care among parents with psychotic disorders. Psychiatr Serv 50:1354–1356. https://doi.org/10.1176/ps.50.10.1354
Schrank B, Rumpold T, Gmeiner A, Priebe S, Aigner M (2016) Parenthood among people with psychotic disorders: gender differences in a non-selective clinical sample. Psychiatry Res 246:474–479. https://doi.org/10.1016/j.psychres.2016.10.020
Fernandes AC, Cloete D, Broadbent MTM, Hayes RD, Chang CK, Jackson RG et al (2013) Development and evaluation of a de-identification procedure for a case register sourced from mental health electronic records. BMC Med Inform Decis Mak. https://doi.org/10.1186/1472-6947-13-71
Stewart R, Soremekun M, Perera G, Broadbent M, Callard F, Denis M et al (2009) The South London and Maudsley NHS Foundation Trust Biomedical Research Centre (SLAM BRC) case register: Development and descriptive data. BMC Psychiatry 9:1–12. https://doi.org/10.1186/1471-244X-9-51
UK Department for Communities and Local Government. The English Indices of Deprivation 2019. 2019.
Choi J, Dekkers OM, le Cessie S (2019) A comparison of different methods to handle missing data in the context of propensity score analysis. Eur J Epidemiol 34:23–36. https://doi.org/10.1007/s10654-018-0447-z
Mcskimming P, Barry S, Park J, Bhattacharya S, Macbeth A. Data linkage of psychiatric and maternity data to investigate the pregnancy outcomes of women with non-affective psychosis in Scotland. Int. J. Popul. Data Sci. 298 Proc. IPDLN Conf. (August 2016), vol. 1, 2017.
Kaplan K, Brusilovskiy E, O’Shea AM, Salzer MS (2019) Child protective service disparities and serious mental illnesses: results from a national survey. Psychiatr Serv 70:202–208. https://doi.org/10.1176/appi.ps.201800277
Mowbray CT, Bybee D, Oyserman D, MacFarlane P (2005) Timing of mental illness onset and motherhood. J Nerv Ment Dis 193:369–378. https://doi.org/10.1097/01.nmd.0000165088.82453.bd
Reininghaus UA, Morgan C, Simpson J, Dazzan P, Morgan K, Doody GA et al (2008) Unemployment, social isolation, achievement-expectation mismatch and psychosis: findings from the ÆSOP Study. Soc Psychiatry Psychiatr Epidemiol 43:743–751. https://doi.org/10.1007/s00127-008-0359-4
Reupert AE, Maybery DJ (2009) Fathers’ experience of parenting with a mental illness. Fam Soc J Contemp Soc Serv 90:61–68. https://doi.org/10.1606/1044-3894.3846
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders (DSM-5). American Psychiatric Pub, New York
Petersen I, Welch CA, Nazareth I, Walters K, Marston L, Morris RW et al (2019) Health indicator recording in UK primary care electronic health records: Key implications for handling missing data. Clin Epidemiol 11:157–167. https://doi.org/10.2147/CLEP.S191437
Royal College of Psychiatrists (2013) Smoking and mental health A joint report by the Royal College of Physicians and the Royal College of Psychiatrists. Smok Ment Heal 2:195–201
Johnson SE, Lawrence D, Perales F, Baxter J, Zubrick SR (2018) Prevalence of mental disorders among children and adolescents of parents with self-reported mental health problems. Community Ment Health J 54:884–897. https://doi.org/10.1007/s10597-017-0217-5
Rasic D, Hajek T, Alda M, Uher R (2014) Risk of mental illness in offspring of parents with schizophrenia, bipolar disorder, and major depressive disorder: a meta-analysis of family high-risk studies. Schizophr Bull 40:28–38. https://doi.org/10.1093/schbul/sbt114
Strand J, Rudolfsson L (2017) A qualitative evaluation of professionals’ experiences of conducting Beardslee’s family intervention in families with parental psychosis. Int J Ment Health Promot 19:289–300. https://doi.org/10.1080/14623730.2017.1345690
Nicholson J, Albert K, Gershenson B, Williams V, Biebel K (2016) Developing family options: outcomes for mothers with severe mental illness at twelve months of participation. Am J Psychiatr Rehabil 19:353–369. https://doi.org/10.1080/15487768.2016.1231639
Gellatly J, Bee P, Kolade A, Hunter D, Gega L, Callender C et al (2019) Developing an intervention to improve the health related quality of life in children and young people with serious parental mental illness. Front Psychiatry 10:1–12. https://doi.org/10.3389/fpsyt.2019.00155
Abel KM, Hope H, Faulds A, Pierce M (2019) Promoting resilience in children and adolescents living with parental mental illness (CAPRI): children are key to identifying solutions. Br J Psychiatry 215:513–515. https://doi.org/10.1192/bjp.2019.118
Foster K, O’Brien L, Korhonen T (2012) Developing resilient children and families when parents have mental illness: a family-focused approach. Int J Ment Health Nurs 21:3–11. https://doi.org/10.1111/j.1447-0349.2011.00754.x
Jewell A, Broadbent M, Hayes RD, Gilbert R, Stewart R, Downs J (2020) Impact of matching error on linked mortality outcome in a data linkage of secondary mental health data with Hospital Episode Statistics (HES) and mortality records in South East London: A cross-sectional study. BMJ Open. https://doi.org/10.1136/bmjopen-2019-035884
Acknowledgements
This research project was supported by the UK Clinical Record Interactive Search (UK-CRIS) system using data and systems of the NIHR Oxford Health Biomedical Research Centre (BRC-1215-20005). We would also like to acknowledge the work and support of the Oxford CRIS Team, Tanya Smith, Head of Research Informatics, Adam Pill, CRIS Academic Support and Information Analyst, Suzanne Fisher, CRIS Academic Support and Information Analyst, Lulu Kane CRIS Administrator. Thank you also to Dr Stephen Puntis for his guidance on the initial design of this study. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. The authors would also like to thank the consultancy service from the Department of Statistics, University of Oxford, and Rachel Pearson, for their advice on the analyses.
Funding
Jessica Radley is a DPhil student and is funded by Mental Health Research UK. No funding was received for conducting this study.
Author information
Authors and Affiliations
Contributions
All the authors contributed to the study conception and design. Data collection and analysis were performed by JR. The first draft of the manuscript was written by JR and all the authors commented on previous versions of the manuscript. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
The use of UK-CRIS for analysis of anonymised secondary data has been approved by the National Health Service Health Research Authority (HRA) and ethical approval is not required for individual studies. This CRIS project was submitted to an independent CRIS Oversight Group for approval.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Radley, J., Barlow, J. & Johns, L.C. Sociodemographic characteristics associated with parenthood amongst patients with a psychotic diagnosis: a cross-sectional study using patient clinical records. Soc Psychiatry Psychiatr Epidemiol 57, 1897–1906 (2022). https://doi.org/10.1007/s00127-022-02279-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-022-02279-x