
Abstract
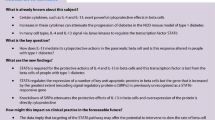
Aims/hypothesis
Inflammation induces beta cell dysfunction and demise but underlying molecular mechanisms remain unclear. The apolipoprotein L (APOL) family of genes has been associated with innate immunity and apoptosis in non-pancreatic cell types, but also with metabolic syndrome and type 2 diabetes mellitus. Here, we hypothesised that APOL genes play a role in inflammation-induced beta cell damage.
Methods
We used single-cell transcriptomics datasets of primary human pancreatic islet cells to study the expression of APOL genes upon specific stress conditions. Validation of the findings was carried out in EndoC-βH1 cells and primary human islets. Finally, we performed loss- and gain-of-function experiments to investigate the role of APOL genes in beta cells.
Results
APOL genes are expressed in primary human beta cells and APOL1, 2 and 6 are strongly upregulated upon inflammation via the Janus kinase (JAK)−signal transducer and activator of transcription (STAT) pathway. APOL1 overexpression increases endoplasmic reticulum stress while APOL1 knockdown prevents cytokine-induced beta cell death and interferon-associated response. Furthermore, we found that APOL genes are upregulated in beta cells from donors with type 2 diabetes compared with donors without diabetes mellitus.
Conclusions/interpretation
APOLs are novel regulators of islet inflammation and may contribute to beta cell damage during the development of diabetes.
Data availability
scRNAseq data generated by our laboratory and used in this study are available in the Gene Expression Omnibus (GEO; www.ncbi.nlm.nih.gov/geo/), accession number GSE218316.
Graphical Abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.

Introduction
Inflammation is one of the most studied causes of beta cell failure. Specifically, exposure to proinflammatory cytokines has been shown to impair beta cell function and increase beta cell death [1,2,3]. Cytokine-induced beta cell damage is regulated via a broad spectrum of pathways. IL-1β can induce inflammation and eventually cell death via NF-κB activation and expression of proinflammatory genes (e.g. iNOS [also known as NOS2] and CXCL10) [4]. IFNγ activates the Janus kinase (JAK)−signal transducer and activator of transcription (STAT) pathway, which leads to STAT translocation to the nucleus and upregulation of target inflammation genes (e.g. interferon regulatory factors [IRFs]) [5, 6]. In addition, the combination of IFNγ + IL-1β can also trigger cell death via the endoplasmic reticulum (ER) stress pathway and the increase in the pro-apoptotic genes ATF3 and CHOP [7, 8]. In a vicious cycle, the cytokine-induced expression of proinflammatory genes via the different pathways mentioned can also lead to the amplification of inflammatory signalling and contribute to cell death.
Targeting inflammation-related pathways has already shown promise for protecting beta cells in the context of both type 1 diabetes mellitus [9, 10] and type 2 diabetes mellitus [11,12,13]. For example, low-dose IL-2 treatment in children with recently diagnosed type 1 diabetes resulted in maintained C-peptide production over 1 year [9]. Interestingly, the combination therapy of liraglutide (a glucagon-like peptide 1 [GLP-1] analogue) and anti-IL-21 antibody resulted in enhanced C-peptide secretion over 54 weeks in adults with recent-onset type 1 diabetes [10]. In the field of type 2 diabetes, blockade of IL-1β with IL-1 receptor antagonists reduced inflammation and improved and/or prevented diabetes in a rat model of type 2 diabetes [11], high-fat diet-fed mice [12] and in individuals with type 2 diabetes [13]. Therefore, the identification of novel targets involved in inflammation-related beta cell damage is relevant for the design of novel therapeutic treatments that could prevent or attenuate beta cell failure in both main types of diabetes.
Apolipoprotein L (APOL) genes belong to a conserved gene family involved in innate immunity. In humans, this gene family codes for six structurally similar proteins (APOL1–6). APOL gene expression is induced by innate immunity-related pathways such as interferons [14,15,16], polyinosinic:polycytidylic acid [poly(I:C)] in endothelial cells and lipopolysaccharides in podocytes [17], among other cell types. The most well-studied APOL protein is APOL1, and it contains a pore-forming domain (PFD) that consists of a BCL2 homology domain 3 (BH3)-motif, a membrane-address domain (MAD) and a serum resistant-associated (SRA) domain [18, 19]. In addition, APOL1 has a signal peptide domain that enables its secretion extracellularly [20]. Functions associated with the APOL family include lipid transport [21, 22], mitochondria-regulated apoptosis [23, 24] and autophagy [25, 26]. In addition, APOL1 risk variants cause lysosomal cell death and cell membrane pore formation, as part of their cell defence mechanism against Trypanosoma infection [18, 19]. Evidence linking APOLs and diabetes is still very scarce. Croyal et al recently reported a positive association between basal serum APOL1 levels and the risk of developing type 2 diabetes [27]. This was in agreement with previous studies in which an association was found between APOL1 concentrations and plasma triglycerides [28] and/or the metabolic syndrome [29].
While the presence of APOL genes has been reported in the pancreas [30], its putative role in beta cell function and the onset or progression of diabetes remains unknown. Here, we have investigated the effect of APOL during inflammation-induced beta cell damage.
Methods
Human islets and cell lines
Human islets were isolated from pancreases of cadaveric donors through the Eurotransplant multiorgan donation programme. Islets were used for research only if they could not be used for clinical purposes, and if research consent was present, according to Dutch National Laws. Human islets with a purity >80% were cultured in ultra-low attachment plates (Corning ref. 3471, USA) with CMRL 1066 (Corning, 99-663-CV, 5 mmol/l glucose), supplemented with 10% FCS, 2 mmol/l l-glutamine, 100 U/ml penicillin, 100 µg/ml streptomycin, 50 µg/ml gentamycin, 20 µg/ml ciprofloxacin, 10 mmol/l HEPES and 1.2 mg/ml nicotinamide. Donor characteristics are listed in electronic supplementary material (ESM) Table 1. Donors were considered to have type 2 diabetes if a history of diabetes was recorded, and/or the HbA1c level was >48 mmol/mol (6.5%) and there was no indication of other types of diabetes mellitus. Donors were considered to have prediabetes if the HbA1c level was between 39 mmol/mol (5.7%) and 46 mmol/mol (6.4%), according to the ADA guidelines [31].
The EndoC-βH1 cell line [32] was obtained from Univercell Biosolutions (Toulouse, France). Cells were seeded in ECM/fibronectin coated plates and cultured with low glucose DMEM (Invitrogen, USA) supplemented with 10 mmol/l nicotinamide, 5.5 g/ml transferrin, 6.7 ng/ml selenite, penicillin-streptomycin and 50 μmol/l β-mercaptoethanol.
HEK293T cells (ATCC, CRL-3216) were cultured in DMEM + 10% FCS. All cell lines are regularly checked for potential mycoplasma infection in our laboratory.
Induction of stress conditions
Human islets were exposed for 24 h or 72 h to 1 ng/ml IL-1β (401-ML, R&D systems) + 50 ng/ml IFNγ (285-IF, R&D systems, USA) (cytokines). EndoC-βH1 cells were treated for 24 h or 72 h with 1 ng/ml IL-1β + IFNγ 50 ng/ml (cytokines), 1, 2 or 4 µmol/l baricitinib (a JAK–STAT inhibitor, HY-15315, MedChemExpress, USA) and 1, 2.5 or 5 µmol/l Bay 11-7082 (196871, Merck, Germany) or 50 µg/ml salicylate (S3007, Merck) (NF-κB inhibitors).
Single-cell RNA-sequencing
We used our single-cell RNA-sequencing Gene Expression Omnibus (GEO; www.ncbi.nlm.nih.gov/geo/) dataset generated from human pancreatic islets treated with beta cell stressors (GSE218316) and performed a differential gene expression analysis of human islet cells treated with IL-1β + IFNγ using a Wilcoxon rank-sum test. We considered genes to be significantly altered if they had an adjusted p value (based on Bonferroni correction) <0.05.
Transcriptomic analysis of type 2 diabetes datasets
Four previously published SMART-seq (GEO GSE83139 [33], GSE81608 [34]) or SMART-seq2 (GEO GSE81547 [35], European Bioinformatics Institute E-MTAB-5061 [36]) scRNA-seq datasets of human pancreatic islets were selected for analysis. Differential gene expression in islets from donors without diabetes and with type 2 diabetes was statistically computed using an unpaired t test. See ESM Methods section for details.
Cell-death staining
Cell death was assessed by using the ReadyProbes Cell Viability Imaging Kit (R37610, Thermo Fisher, USA). EndoC-βH1 cells were incubated with propidium iodide (PI) and Hoechst 33342 for 20 min and imaged with the ImageXpress confocal microscope (Molecular Devices, USA). Blinded quantification was performed with Fiji (2016, https://imagej.net/software/fiji/downloads) by using a nucleus-counting macro.
RT-qPCR
RNA (250–500 ng) was obtained from human islets and EndoC-βH1 cells by cell lysis with RLT buffer with β-mercaptoethanol according to the manufacturer’s instructions (micro RNeasy kit from Qiagen, Hilden, Germany). Isolated RNA was reverse-transcribed to DNA with M-MLV reverse transcriptase (Invitrogen), oligo(dT)s (Qiagen), dNTP (Promega, USA), DTT (Invitrogen) and RNAse-OUT (ThermoFisher). Quantitative PCR (qPCR) was performed with IQ SYBR green mix (170–8887, Bio-Rad, Hercules, USA). GAPDH and ACTB were used as housekeeping genes. Amplification and detection were performed by using CFX systems (Bio-Rad) and fold changes were obtained by using the \({2}^{{-\Delta \Delta \mathrm{C}}_{\mathrm{t}}}\) method. Primers are included in ESM Table 2.
Immunohistochemistry and fluorescence microscopy
Coverslip-cultured EndoC-βH1 cells, isolated human islets or pancreatic tissue samples were fixed in 4% formaldehyde solution and embedded in 2% agar and paraffin. Samples were sectioned into 4 μm slides using the Leica microtome (RM2255, Leica, Germany). Slides were deparaffinised and rehydrated. Blocking was done with 5% normal donkey serum followed by primary and secondary antibody incubations. For nuclei staining, an extra step with 1% Triton X-100 was performed. Immunofluorescence was detected with a Leica microscope (Leica SP8). Antibodies used are listed in ESM Table 3.
Western blotting
After treatment, approximately 3.000 islet equivalents or 350.000 EndoC-βH1 cells were washed with cold PBS and lysed in RIPA lysis and extraction buffer with 1/100 protease and phosphatase inhibitor (Thermo Fisher). Lysates were passed ten times with a 26-gauge needle and centrifuged to obtain the supernatant. Protein content was measured by BCA protein content kit (Thermo Fisher) and 10–20 μg protein was loaded in 12% mini-PROTEAN TGX gels (Bio-Rad) and transferred to 0.2 µmol/l PVDF membranes (Trans-blot turbo mini 0.2 µmol/l PVDF transfer packs, Bio-Rad). Membranes were blocked with 5% Milk in PBS-Tween for 1 h, incubated with primary antibody overnight at 4°C, and after three washes with PBS-Tween, incubated for 1 h with secondary antibody at room temperature. Primary and secondary antibodies were diluted in the same buffer as the one used for blocking the membrane. Blots were incubated with Supersignal West Pico PLUS Chemiluminescent substrate (Thermo Fisher), visualised with Bio-Rad ChemiDoc Touch (Bio-Rad) and analysed with Image Lab (version 6.1, Bio-Rad). Antibodies used are listed in ESM Table 3.
Lentivirus-mediated overexpression and knockdown
For overexpression, open reading frames (ORFs) of APOL1 and APOL2 in pDONR223 vector were picked from the MISSION TRC3 Human LentiORF Collection (Sigma-Aldrich), amplified by PCR using the following primers: APOL1 forward (XhoI): TTCTCGAGATGGAGGGAGCTG; APOL1 reverse (XbaI): AATCTAGAGGCTTGTGTCCACC; APOL2 forward (XhoI): TTCTCGAGATGAATCCAGAGAGC; APOL2 reverse (XbaI): AATCTAGATTGGTCTTGGCCTGGC; and subsequently subcloned into pLV-CMV-IRES-puro vector (XhoI/XbaI) for expression. All constructs were verified by sequencing.
The shRNA lentiviral constructs against APOL1, APOL2 and APOL6 were obtained from the MISSION shRNA library (clones TRCN118633, TRCN83107, TRCN151077, Sigma-Aldrich) and produced as described previously [37].
For transduction, EndoC-βH1 cells were infected with a multiplicity of infection (MOI) of 1 in DMEM/polybrene overnight. After, cells were washed in PBS and replaced with fresh DMEM for 48 h or 72 h, for overexpression or knockdown experiments, respectively.
siRNA-mediated knockdown
EndoC-βH1 cells were transfected overnight with 30 nmol/l siRNA targeting human STAT1 (ON-target SMARTpool human siSTAT1, L-003543-00, Horizon Discovery, Cambridge, UK), or non-target control (ON-TARGETplus Non-targeting siRNAs, D-001810-01, Horizon Discovery). Transfection was performed with Dharmafect transfection reagent (Horizon Discovery) as described in the manufacturer’s instructions. After 48 h, cytokines were added for 24 h.
Statistics
Results are represented as mean ± SEM. Comparisons were performed by two-tailed student t test and a p value <0.05 was considered significant.
Results
APOL genes are expressed in primary human beta cells and upregulated upon inflammation
We first set out to determine whether APOL genes are expressed in primary human pancreatic beta cells using our single-cell RNA-seq dataset from primary human islets exposed to diverse metabolic and inflammatory stressors in parallel: glucose (22 mmol/l) + palmitate (0.5 mmol/l), thapsigargin (0.1 µmol/l), IL-1β (1 ng/ml) + IFNγ (1000 U/ml), IFNα (2000 U/ml), fibroblast growth factor 2 (FGF2; 100 ng/ml) or hypoxia for 24 h and 72 h.
In the untreated condition, APOL2 and 6 were the most highly expressed in beta cells (Fig. 1a). Upon IL-1β + IFNγ treatment APOL1, APOL2 and APOL6 gene expression was significantly increased in beta cells, and APOL2 and APOL6 was increased in IFNα-treated cells. By contrast, no upregulation of APOL genes was found in beta cells exposed to glucose + palmitate, thapsigargin, hypoxia or FGF2 treatments (Fig. 1a and ESM Table 4).

Cytokines increase APOL expression in human islets and beta cells. (a) Dotplot from scRNA-seq analysis shows the mean and percentage expression of APOL genes in beta cells exposed to different stressors for 24 h and 72 h (merged timepoints). Human islets (b, e) and EndoC-βH1 cells (c, d, e) were treated with IL-1β + IFNγ (Cytokines) for 24 h and 72 h. (b–e) Gene and protein expression of APOL1, APOL2 and APOL6 were determined by qPCR (b, c), western blot (d) and immunofluorescence staining (e). ACTB and GAPDH were used to normalise mRNA expression and tubulin was used as loading control for western blots. (e) Fluorescence double staining of APOL proteins (green) and DAPI for nuclei (blue) was performed in EndoC-βH1 cells and human islets. Scale bar, 100 µm. (b, c) Results are the means ± SEM of 3–6 independent experiments; **p<0.01, ***p<0.001, by paired (b) or unpaired (c) Student’s t test
Cytokine-induced expression of APOL1, APOL2 and APOL6 was validated by qPCR in human islets (Fig. 1b) and EndoC-βH1 cells (Fig. 1c) exposed to IL-1β + IFNγ. In addition, we found a significant upregulation of APOL1, APOL2 and APOL6 protein levels upon inflammation in EndoC-βH1 cells by western blot (Fig. 1d) and by immunostaining in both EndoC-βH1 cells and primary human beta cells (Fig. 1e). Of note, there is no effect of time in culture (with or without cytokines) on APOL gene expression (ESM Fig 1a, b and d).
Finally, we assessed the contribution of individual cytokines on the induction of APOL genes in beta cells, and we found that APOL genes are mainly upregulated by IFNγ (ESM Fig. 1c).
Together, these data reveal that APOL1, APOL2 and APOL6 are specifically upregulated by inflammation in human beta cells.
Cytokine-induced APOL expression is mediated by the JAK–STAT pathway
We next investigated which of the main inflammation-induced signalling pathways mediates the upregulation of APOL genes in human beta cells. NF-κB pathway inhibition by salicylate or Bay 11-7082 did not affect cytokine-induced expression of APOL1, APOL2 or APOL6 (Fig. 2a), but blocked TNFA (also known as TNF) gene expression as expected (ESM Fig. 2a).

APOL expression is regulated by the JAK–STAT pathway. (a, b) EndoC-βH1 cells were exposed to IL-1β + IFNγ (Cytokines) for 72 h, alone or in combination with Bay 11-7082/salicylate (NF-κB inhibitors) (a) or 4 μmol/l baricitinib (JAK–STAT inhibitor) (b). (c, d) EndoC-βH1 cells were transfected with siSTAT1 or non-targeting siRNA (Mock). After 48 h, the cells were subjected to 24 h cytokine treatment (IL-1β + IFNγ). Gene expression of STAT1 and IRF1 (c) and APOL1, APOL2 and APOL6 (d) was analysed by qPCR and normalised to housekeeping genes GAPDH and ACTB. Results are the means ± SEM of 2–5 independent experiments; *p<0.05; **p<0.01, ***p<0.001, by unpaired Student’s t test
On the other hand, treatment with the JAK–STAT inhibitor baricitinib abolished cytokine-induced APOL1/APOL2/APOL6 expression significantly both at 24 h and 72 h (Fig. 2b), as well as the IFNγ-response genes MX1, HLA-ABC and TNFA as expected (ESM Fig. 2b).
In order to confirm the involvement of the JAK–STAT pathway, we specifically targeted STAT1 using siRNA. STAT1 gene expression was very efficiently downregulated, resulting in reduced expression of its target gene IRF1 (Fig. 2c). Furthermore, cytokine-induced upregulation of APOL1 and 2 was strongly prevented upon downregulation of STAT1 (Fig. 2d).
APOL gene overexpression upregulates ER stress
To investigate the role of APOL genes in beta cells, we overexpressed APOL1 and APOL2 by lentiviral transduction in EndoC-βH1 cells (Fig. 3a). We observed a trend towards an increased cell death for both APOL genes even though the differences failed to reach statistical difference (p=0.06 [APOL1] and p=0.08 [APOL2]) (Fig. 3b,c).

APOL overexpression regulates beta cell death. EndoC-βH1 cells were transfected with control empty vector CMV-GFP (black bars) or overexpression constructs for APOL1 (light blue) or APOL2 (dark blue). (a, d) Gene expression was analysed by qPCR and normalised to housekeeping genes GAPDH and ACTB. (b, c) Cell death was assessed by propidium iodide (PI; red)/Hoechst (blue) staining (b) and quantified with ImageJ (c). Scale bar, 500 µm. Results are the means ± SEM of 3–4 independent experiments; *p<0.05, **p<0.01, ***p<0.001 by paired Student’s t test compared with the CMV-GFP condition
In addition, APOL1 upregulation led to a significant increase of the pro-apoptotic ER stress genes ATF3 and CHOP at 48 h post-transduction (Fig. 3d). Along the same lines, we observed an increase in ATF3 expression with APOL1 and 2 overexpression in HEK293T cells (ESM Fig. 3a,b). No change in the protein levels of phosphorylated STAT1 was found upon APOL1 or APOL2 overexpression, which indicates overall no change in JAK–STAT pathway activation (ESM Fig. 3c, d). Of note, ATF3 was also found to be upregulated upon cytokine treatment (ESM Fig. 4a,b,c).
APOL1 downregulation prevents cytokine-induced beta cell death and interferon-associated response
Our data so far revealed that APOL genes are upregulated upon inflammation and that they could have a detrimental effect on human beta cells. We therefore investigated whether APOL gene downregulation could protect against cytokine-induced beta cell damage. We knocked down APOL1, APOL2 or APOL6 gene expression in cytokine-treated EndoC-βH1 cells leading to a >80% reduced expression of all three genes (Fig. 4a). Strikingly, we found that downregulation of APOL1 abolished cytokine-induced beta cell death (Fig. 4b,c). This effect was associated with a reduced expression of the cytokine-induced pro-apoptotic ER stress markers ATF3 and CHOP by 39% and 33% via APOL1 knockdown (Fig. 4d).

APOL1 knockdown reduces cytokine-induced cell death and expression of ER stress genes in EndoC-βH1. EndoC-βH1 cells were transfected with shCtrl (black bars) or shRNAs targeting APOL1 (green), APOL2 (dark purple) or APOL6 (light purple) after 72 h of cytokine treatment (IL-1β + IFNγ). Gene expression (a, d, e, g) was analysed by qPCR and normalised to housekeeping genes GAPDH and ACTIN (n=4–5). (b, c) Cell death was assessed by propidium iodide (PI; red)/Hoechst (blue) staining (b) and quantified with ImageJ (c). Scale bar, 500 µm. (f) Protein levels of phospho-STAT1 (Tyr701) (p-STAT1), total STAT1 (STAT1) and GAPDH (as loading control) were analysed by western blotting and quantified. Results are the means ± SEM of 3–5 independent experiments. *p<0.05, **p<0.01, ***p<0.001, by paired Student’s t test compared with the indicated condition
Next, we checked the expression of mediators and target genes of the interferon response. We found that cytokine-induced IRF1 and STAT1 expression was significantly reduced by APOL1 knockdown (34% and 50%, respectively) and IRF1 by APOL2 knockdown (48%) (Fig. 4e). APOL6 knockdown did not decrease the expression of the aforementioned genes. In line with gene expression data, exposure to IL-1β + IFNγ increased phosphorylated STAT1, but this was not significantly decreased by APOL1 and APOL2 knockdown (Fig. 4f). Finally, APOL1 downregulation prevented the increase in inflammation-induced expression of target genes MX1 and HLA-ABC by 35% and 27%, respectively (Fig. 4g).
APOL genes are upregulated in human beta cells from donors with type 2 diabetes
Finally, we asked whether these findings have any significance in pathophysiological conditions. We merged and analysed four publicly available single-cell transcriptomic datasets of primary human islet cells from donors with type 2 diabetes [33,34,35,36] (Fig. 5a, ESM Fig. 5a). APOL2 and 6 genes were the most highly expressed in beta cells from donors without diabetes, while expression of APOL1, APOL3 and APOL4 in beta cells was very low and APOL5 was undetectable (Fig. 5b; ESM Fig. 5b and data not shown).

APOL family members are upregulated in islets from donors with type 2 diabetes. (a) Schematic representation of the transcriptomic analysis data used to study gene expression in beta cells from donors with type 2 diabetes (T2DM; n=12) in comparison with donors without diabetes (no diabetes [ND]; n=24); datasets from [33,34,35,36]. Created with BioRender.com. (b) Violin plots showing gene expression for different APOL genes in beta cells from donors without diabetes. (c) Volcano plot representing the differential expression of APOL genes in donors with type 2 diabetes. (d–f) APOL1, APOL2 and APOL6 protein expression determination by western blotting (d, e) in islets from donors without diabetes (ND; n=3) and with (pre)diabetes (preDM/T2DM; n=3). Fluorescence microscopy (f) of APOL1, APOL2 and APOL6 (green), C-peptide (red) and DAPI for nuclei (blue) in islets from donors with type 2 diabetes (T2DM) and without diabetes (ND). Scale bar, 50 µm. Results are the means ± SEM of three independent experiments (d, e); *p<0.05, by unpaired Student’s t test
Furthermore, we found that APOL 2, 4 and 6 were significantly upregulated in beta cells from donors with type 2 diabetes compared with donors without diabetes (Fig. 5c; ESM Table 4). Interestingly, additional pathway analysis (ESM Fig. 5d,e) showed an enrichment of the interferon pathway in beta cells from the donors with type 2 diabetes analysed compared with donors without diabetes mellitus. Some over-represented genes found were STAT2, IRF9 and IFI6, all interferon-regulated genes.
Next, we assessed APOL1, 2 and 6 protein expression by western blot in isolated human islets obtained in our facility (Fig. 5d,e). We observed a significantly higher protein expression of APOL1 by 12.8-fold in islets from three donors with (pre-)diabetes, while APOL2 and APOL6 were not significantly altered in these donors. The increase in APOL1 was confirmed by immunostaining in a pancreas section of another donor with type 2 diabetes (Fig. 5f). APOL2 and APOL6 were also found to be upregulated in beta cells of this donor.
Of note, the upregulation of APOL genes was not restricted to beta cells as it was also seen in the single-cell RNA-seq data (see ESM Fig. 5c and ESM Table 5).
Overall, despite inter-donor differences, we found an upregulation of APOL genes in beta cells of donors with a history of type 2 diabetes.
Discussion
Here, we show that APOL genes are expressed in human pancreatic beta cells and expression of APOL1, 2 and 6 is upregulated upon inflammatory conditions. Furthermore, we propose that APOL gene upregulation plays a role in the amplification of inflammation in beta cells.
APOL gene expression was significantly increased upon cytokine stress, particularly by IFNγ, but not upon other ER stress conditions such as thapsigargin, high glucose or palmitate, which are associated with beta cell dysfunction and/or damage. The results from this study point towards a specific inflammatory regulation of this gene family, in agreement with observations in other cell types where APOL genes were also reported as interferon-response genes [15, 17, 26, 37,38,39].
Moreover, we uncovered that APOL genes are upregulated in beta cells from patients with type 2 diabetes mellitus, a condition associated with low-grade inflammation. This is in line with recent studies reporting an association between APOL1 levels in serum and increased risk of type 2 diabetes [27] and the metabolic syndrome [29]. Whether an increase in APOL genes can (negatively) influence insulin secretion and contribute to the inflammation-induced beta cell dysfunction that occurs in type 2 diabetes remains to be further investigated. In addition, this study was focused on the role of endogenous APOL genes in beta cells. Future studies assessing the impact of exogenous APOL1 on beta cells could contribute to the understanding of the role of elevated APOL1 levels in serum, which are associated with type 2 diabetes risk [27].
We found that APOL1, APOL2 and APOL6 expression in human beta cells is mediated by the inflammatory JAK–STAT pathway. Other studies have shown that Sp1, IRF1 and IRF2 can bind to the APOL1 promoter in hepatoma cells [40], and IRF1, IRF2 and STAT2 to the APOL1 promoter in podocytes and endothelial cells [17]. In addition, the authors of this latter study showed that NF-κB inhibitors downregulate poly(I:C)-induced APOL1 expression, although NF-κB subunits did not bind to the APOL1 promoter directly [17]. In our study, we did not observe a role for the NF-κB pathway in regulating APOL gene expression. However, we found that downregulation of APOL1 and APOL2 in cytokine-treated beta cells was associated with a decrease in IRF1 and STAT1 both at gene and protein levels.
Importantly, ER stress is one of the factors that contributes to the loss of beta cell function in both type 1 diabetes [41] and type 2 diabetes [42], as well as promoting beta cell death [43]. In this study, we showed that APOL1 or APOL2 overexpression led to a modest increase in the pro-apoptotic ER stress genes ATF3 and CHOP in EndoC-βH1 cells, and a much stronger induction in HEK293T cells. By contrast, downregulation of APOL1 gene expression prevented cytokine-induced apoptosis, paralleled by a decrease in ER stress and inflammatory gene expression. A direct contribution of wild type APOL genes on induction of ER stress in beta cells will require more evidence, especially in other models, including primary human beta cells. Previous studies have reported that APOL1 risk variants can induce ER stress in human podocytes [44] and podocyte-like cells from Drosophila [45]. Interestingly, inhibition of ER stress likewise prevented APOL1-mediated cell death [44, 45]. APOL gene overexpression, especially APOL1 and APOL6, has been reported to promote apoptosis in embryonic kidney cells [46], podocytes [47] and colorectal cancer cell lines [24].
APOL2 downregulation resulted in a decrease in ER stress and inflammation, while no change was detected in beta cell death. APOL2 has been reported to have an anti-apoptotic role in human bronchial epithelial cells [14] and HeLa cells [15]. Our results also contrast with the work from Liao et al, which showed that APOL2 knockdown sensitised cells to IFNγ cytotoxicity [14], while Galindo-Moreno et al found no effect of APOL2 knockdown in IFNγ-induced cell death [15]. Thus the function of APOL genes may be partly cell-type specific.
The results from this study indicate that APOL1, APOL2 and APOL6 are overall detrimental. While the role of APOL1 appears to be pro-apoptotic in this and previous work, more studies are needed to decipher the role of other APOLs such as APOL2 and APOL6. Of note, we observed that the APOL2 expression levels of untreated control beta cells were higher in comparison with other APOL genes. Thus, the presence of APOL2 might be important in maintaining beta cell health up to a certain threshold, after which it could become toxic and eventually trigger cell death. Regarding APOL6, earlier studies showed that knockdown inhibited IFNγ-induced apoptosis in atherosclerotic muscle cells [26], implying a negative role for this gene. Yet, we only found a moderate decrease on the levels of ER stress and inflammatory genes upon downregulation of APOL6 in beta cells exposed to cytokines.
Overall, this study uncovers APOLs as a new gene family that has an implication in beta cell inflammation, and therefore potentially in the onset and/or progression of diabetes mellitus. In conclusion, APOLs appear to be relevant in beta cell health and stress and may be promising targets for reducing progressive beta cell failure.
Abbreviations
- APOL:
-
Apolipoprotein L
- ER stress:
-
Endoplasmic reticulum stress
- FGF2:
-
Fibroblast growth factor 2
- IRF:
-
Interferon regulatory factor
- JAK:
-
Janus kinase
- PI:
-
Propidium iodide
- qPCR:
-
Quantitative PCR
- STAT:
-
Signal transducer and activator of transcription
References
Grunnet LG, Aikin R, Tonnesen MF et al (2009) Proinflammatory cytokines activate the intrinsic apoptotic pathway in beta-cells. Diabetes 58(8):1807–1815. https://doi.org/10.2337/db08-0178
Burke SJ, Stadler K, Lu D et al (2015) IL-1beta reciprocally regulates chemokine and insulin secretion in pancreatic beta-cells via NF-kappaB. Am J Physiol Endocrinol Metab 309(8):E715-726. https://doi.org/10.1152/ajpendo.00153.2015
Dettmer R, Niwolik I, Cirksena K et al (2022) Proinflammatory cytokines induce rapid, NO-independent apoptosis, expression of chemotactic mediators and interleukin-32 secretion in human pluripotent stem cell-derived beta cells. Diabetologia 65(5):829–843. https://doi.org/10.1007/s00125-022-05654-0
Pedersen SS, Prause M, Williams K, Barres R, Billestrup N (2022) Butyrate inhibits IL-1beta-induced inflammatory gene expression by suppression of NF-kappaB activity in pancreatic beta cells. J Biol Chem 298(9):102312. https://doi.org/10.1016/j.jbc.2022.102312
Moore F, Naamane N, Colli ML et al (2011) STAT1 is a master regulator of pancreatic beta-cell apoptosis and islet inflammation. J Biol Chem 286(2):929–941. https://doi.org/10.1074/jbc.M110.162131
Nardelli TR, Vanzela EC, Benedicto KC et al (2018) Prolactin protects against cytokine-induced beta-cell death by NFkappaB and JNK inhibition. J Mol Endocrinol 61(1):25–36. https://doi.org/10.1530/JME-16-0257
Brozzi F, Nardelli TR, Lopes M et al (2015) Cytokines induce endoplasmic reticulum stress in human, rat and mouse beta cells via different mechanisms. Diabetologia 58(10):2307–2316. https://doi.org/10.1007/s00125-015-3669-6
Cardozo AK, Ortis F, Storling J et al (2005) Cytokines downregulate the sarcoendoplasmic reticulum pump Ca2+ ATPase 2b and deplete endoplasmic reticulum Ca2+, leading to induction of endoplasmic reticulum stress in pancreatic beta-cells. Diabetes 54(2):452–461. https://doi.org/10.2337/diabetes.54.2.452
Rosenzwajg M, Salet R, Lorenzon R et al (2020) Low-dose IL-2 in children with recently diagnosed type 1 diabetes: a phase I/II randomised, double-blind, placebo-controlled, dose-finding study. Diabetologia 63(9):1808–1821. https://doi.org/10.1007/s00125-020-05200-w
von Herrath M, Bain SC, Bode B et al (2021) Anti-interleukin-21 antibody and liraglutide for the preservation of beta-cell function in adults with recent-onset type 1 diabetes: a randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Diabetes Endocrinol 9(4):212–224. https://doi.org/10.1016/S2213-8587(21)00019-X
Ehses JA, Lacraz G, Giroix MH et al (2009) IL-1 antagonism reduces hyperglycemia and tissue inflammation in the type 2 diabetic GK rat. Proc Natl Acad Sci U S A 106(33):13998–14003. https://doi.org/10.1073/pnas.0810087106
Sauter NS, Schulthess FT, Galasso R, Castellani LW, Maedler K (2008) The antiinflammatory cytokine interleukin-1 receptor antagonist protects from high-fat diet-induced hyperglycemia. Endocrinology 149(5):2208–2218. https://doi.org/10.1210/en.2007-1059
Larsen CM, Faulenbach M, Vaag A et al (2007) Interleukin-1-receptor antagonist in type 2 diabetes mellitus. N Engl J Med 356(15):1517–1526. https://doi.org/10.1056/NEJMoa065213
Liao W, Goh FY, Betts RJ et al (2011) A novel anti-apoptotic role for apolipoprotein L2 in IFN-gamma-induced cytotoxicity in human bronchial epithelial cells. J Cell Physiol 226(2):397–406. https://doi.org/10.1002/jcp.22345
Galindo-Moreno J, Iurlaro R, El Mjiyad N, Diez-Perez J, Gabaldon T, Munoz-Pinedo C (2014) Apolipoprotein L2 contains a BH3-like domain but it does not behave as a BH3-only protein. Cell Death Dis 5(6):e1275. https://doi.org/10.1038/cddis.2014.237
Zhaorigetu S, Wan G, Kaini R, Jiang Z, Hu CA (2008) ApoL1, a BH3-only lipid-binding protein, induces autophagic cell death. Autophagy 4(8):1079–1082. https://doi.org/10.4161/auto.7066
Nichols B, Jog P, Lee JH et al (2015) Innate immunity pathways regulate the nephropathy gene Apolipoprotein L1. Kidney Int 87(2):332–342. https://doi.org/10.1038/ki.2014.270
Perez-Morga D, Vanhollebeke B, Paturiaux-Hanocq F et al (2005) Apolipoprotein L-I promotes trypanosome lysis by forming pores in lysosomal membranes. Science 309(5733):469–472. https://doi.org/10.1126/science.1114566
Thomson R, Genovese G, Canon C et al (2014) Evolution of the primate trypanolytic factor APOL1. Proc Natl Acad Sci U S A 111(20):E2130-2139. https://doi.org/10.1073/pnas.1400699111
Page NM, Butlin DJ, Lomthaisong K, Lowry PJ (2001) The human apolipoprotein L gene cluster: identification, classification, and sites of distribution. Genomics 74(1):71–78. https://doi.org/10.1006/geno.2001.6534
Albert TS, Duchateau PN, Deeb SS et al (2005) Apolipoprotein L-I is positively associated with hyperglycemia and plasma triglycerides in CAD patients with low HDL. J Lipid Res 46(3):469–474. https://doi.org/10.1194/jlr.M400304-JLR200
Valsecchi M, Cazzetta V, Oriolo F et al (2020) APOL1 polymorphism modulates sphingolipid profile of human podocytes. Glycoconj J 37(6):729–744. https://doi.org/10.1007/s10719-020-09944-w
Vanwalleghem G, Fontaine F, Lecordier L et al (2015) Coupling of lysosomal and mitochondrial membrane permeabilization in trypanolysis by APOL1. Nat Commun 6:8078. https://doi.org/10.1038/ncomms9078
Liu Z, Lu H, Jiang Z, Pastuszyn A, Hu CA (2005) Apolipoprotein l6, a novel proapoptotic Bcl-2 homology 3-only protein, induces mitochondria-mediated apoptosis in cancer cells. Mol Cancer Res 3(1):21–31. https://doi.org/10.1158/1541-7786.21.3.1
Wan G, Zhaorigetu S, Liu Z, Kaini R, Jiang Z, Hu CA (2008) Apolipoprotein L1, a novel Bcl-2 homology domain 3-only lipid-binding protein, induces autophagic cell death. J Biol Chem 283(31):21540–21549. https://doi.org/10.1074/jbc.M800214200
Zhaorigetu S, Yang Z, Toma I, McCaffrey TA, Hu CA (2011) Apolipoprotein L6, induced in atherosclerotic lesions, promotes apoptosis and blocks Beclin 1-dependent autophagy in atherosclerotic cells. J Biol Chem 286(31):27389–27398. https://doi.org/10.1074/jbc.M110.210245
Croyal M, Wargny M, Chemello K et al (2022) Plasma apolipoprotein concentrations and incident diabetes in subjects with prediabetes. Cardiovasc Diabetol 21(1):21. https://doi.org/10.1186/s12933-022-01452-5
Duchateau PN, Movsesyan I, Yamashita S et al (2000) Plasma apolipoprotein L concentrations correlate with plasma triglycerides and cholesterol levels in normolipidemic, hyperlipidemic, and diabetic subjects. J Lipid Res 41(8):1231–1236. https://doi.org/10.1016/S0022-2275(20)33430-1
Nishimura K, Murakami T, Sakurai T et al (2019) Circulating Apolipoprotein L1 is associated with insulin resistance-induced abnormal lipid metabolism. Sci Rep 9(1):14869. https://doi.org/10.1038/s41598-019-51367-7
Duchateau PN, Pullinger CR, Orellana RE et al (1997) Apolipoprotein L, a new human high density lipoprotein apolipoprotein expressed by the pancreas. Identification, cloning, characterization, and plasma distribution of apolipoprotein L. J Biol Chem 272(41):25576–25582. https://doi.org/10.1074/jbc.272.41.25576
American Diabetes Association (2010) Diagnosis and classification of diabetes mellitus. Diabetes Care 33(Suppl 1):S62-69. https://doi.org/10.2337/dc10-S062
Ravassard P, Hazhouz Y, Pechberty S et al (2011) A genetically engineered human pancreatic beta cell line exhibiting glucose-inducible insulin secretion. J Clin Invest 121(9):3589–3597. https://doi.org/10.1172/JCI58447
Wang YJ, Schug J, Won KJ et al (2016) Single-cell transcriptomics of the human endocrine pancreas. Diabetes 65(10):3028–3038. https://doi.org/10.2337/db16-0405
Xin Y, Kim J, Okamoto H et al (2016) RNA sequencing of single human islet cells reveals type 2 diabetes genes. Cell Metab 24(4):608–615. https://doi.org/10.1016/j.cmet.2016.08.018
Enge M, Arda HE, Mignardi M et al (2017) Single-cell analysis of human pancreas reveals transcriptional signatures of aging and somatic mutation patterns. Cell 171(2):321-330 e314. https://doi.org/10.1016/j.cell.2017.09.004
Segerstolpe A, Palasantza A, Eliasson P et al (2016) Single-cell transcriptome profiling of human pancreatic islets in health and type 2 diabetes. Cell Metab 24(4):593–607. https://doi.org/10.1016/j.cmet.2016.08.020
Carlotti F, Bazuine M, Kekarainen T et al (2004) Lentiviral vectors efficiently transduce quiescent mature 3T3-L1 adipocytes. Mol Ther 9(2):209–217. https://doi.org/10.1016/j.ymthe.2003.11.021
Kreit M, Vertommen D, Gillet L, Michiels T (2015) The interferon-inducible mouse Apolipoprotein L9 and prohibitins cooperate to restrict Theiler’s virus replication. PLoS One 10(7):e0133190. https://doi.org/10.1371/journal.pone.0133190
Gaudet RG, Zhu S, Halder A et al (2021) A human apolipoprotein L with detergent-like activity kills intracellular pathogens. Science 373(6552):eabf8113. https://doi.org/10.1126/science.abf8113
Wang DP, Yu ZX, He ZC et al (2020) Apolipoprotein L1 is transcriptionally regulated by SP1, IRF1 and IRF2 in hepatoma cells. FEBS Lett 594(19):3108–3121. https://doi.org/10.1002/1873-3468.13887
Tersey SA, Nishiki Y, Templin AT et al (2012) Islet beta-cell endoplasmic reticulum stress precedes the onset of type 1 diabetes in the nonobese diabetic mouse model. Diabetes 61(4):818–827. https://doi.org/10.2337/db11-1293
Brusco N, Sebastiani G, Di Giuseppe G et al (2023) Intra-islet insulin synthesis defects are associated with endoplasmic reticulum stress and loss of beta cell identity in human diabetes. Diabetologia 66(2):354–366. https://doi.org/10.1007/s00125-022-05814-2
Laybutt DR, Preston AM, Akerfeldt MC et al (2007) Endoplasmic reticulum stress contributes to beta cell apoptosis in type 2 diabetes. Diabetologia 50(4):752–763. https://doi.org/10.1007/s00125-006-0590-z
Wen H, Kumar V, Lan X et al (2018) APOL1 risk variants cause podocytes injury through enhancing endoplasmic reticulum stress. Biosci Rep 38(4):BSR20171713. https://doi.org/10.1042/BSR20171713
Gerstner L, Chen M, Kampf LL et al (2022) Inhibition of endoplasmic reticulum stress signaling rescues cytotoxicity of human apolipoprotein-L1 risk variants in Drosophila. Kidney Int 101(6):1216–1231. https://doi.org/10.1016/j.kint.2021.12.031
Olabisi OA, Zhang JY, VerPlank L et al (2016) APOL1 kidney disease risk variants cause cytotoxicity by depleting cellular potassium and inducing stress-activated protein kinases. Proc Natl Acad Sci U S A 113(4):830–837. https://doi.org/10.1073/pnas.1522913113
Lan X, Jhaveri A, Cheng K et al (2014) APOL1 risk variants enhance podocyte necrosis through compromising lysosomal membrane permeability. Am J Physiol Renal Physiol 307(3):F326-336. https://doi.org/10.1152/ajprenal.00647.2013
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Acknowledgements
The authors thank R. C. Hoeben and M. Rabelink from the viral vector facility (Dept of Cell & Chemical Biology, Leiden University Medical Center) for the production of lentiviral vectors. We also thank S. du Pré (Dept of Internal Medicine, Leiden University Medical Center) for careful reading of the manuscript.
Data availability
scRNAseq data generated by our laboratory and used in this study are available in the Gene Expression Omnibus (GEO; www.ncbi.nlm.nih.gov/geo/), accession number GSE218316.
Funding
FC and EJPdK have received funding from the DON Foundation, the Dutch Diabetes Research Foundation, JDRF, the Bontius Foundation and the Novo Nordisk Foundation Center for Stem Cell Medicine reNEW (NNF21CC0073729).
Authors’ relationships and activities
The authors declare that there are no relationships or activities that might bias, or be perceived to bias, their work.
Contribution statement
MP-B and FC designed experiments and wrote and revised the manuscript. FC and EJPdK received the funding and contributed to the interpretation of the results. MP-B performed experiments and the analysis and interpretation of the results. AMG and TJJdW performed the RNA-sequencing analysis. NdG, MvA, LD, EvdS, FL and AvdS contributed to performing experiments. AZ contributed to the cloning and generation of lentiviral vectors and to the data interpretation. All authors reviewed the article and approved the final version of the manuscript. FC is the guarantor of this work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Paz-Barba, M., Muñoz Garcia, A., de Winter, T.J.J. et al. Apolipoprotein L genes are novel mediators of inflammation in beta cells. Diabetologia 67, 124–136 (2024). https://doi.org/10.1007/s00125-023-06033-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-023-06033-z