
Abstract
Aims/hypothesis
The aim of this study was to investigate the association between daily life activity and risk of developing diabetes.
Methods
The study population included 2924 Japanese male office workers aged 35 to 59 years who did not have IFG (fasting plasma glucose level 6.1–6.9 mmol/l), Type 2 diabetes (fasting plasma glucose level ≥7.0 mmol/l and/or medication for diabetes) or a history of cardiovascular disease, and were not receiving medication for hypertension. A 1-day activity record during an ordinary weekday was used to estimate daily energy expenditure. Fasting glucose levels were measured at annual health examinations performed in May from 1994 to 2001.
Results
Over a 7-year follow-up period the relative risk of IFG and Type 2 diabetes decreased with increasing daily energy expenditure after controlling for potential predictors of diabetes (p<0.001 and p=0.001 for trend respectively). The age-adjusted relative risk of IFG or Type 2 diabetes decreased with increasing energy expenditure on occupational physical activity, brisk walking, riding on vehicles (standing position) to and from work and other physical activities (all p<0.001 for trend). The association with riding on vehicles (standing position) and other physical activities remained after controlling for other potential confounders of diabetes (p=0.026 and p=0.003 for trend respectively). Results of stratified analyses by the presence or absence of different risk factors for diabetes revealed that the risk of IFG or Type 2 diabetes was inversely related to daily energy expenditure both in men at low risk of diabetes and those at high risk.
Conclusions/interpretation
Physical activity in daily life is inversely associated with the risk of developing IFG or Type 2 diabetes.
Similar content being viewed by others

Introduction
In 1995, there were approximately 135 million individuals with diabetes worldwide, and this number is expected to rise to about 300 million by the year 2025 [1]. A similar increase is anticipated in Japan (from 6.3 to 8.5 million). Although the strongest predisposing factors for Type 2 diabetes are age, obesity and a family history of diabetes [2, 3], evidence is increasing that Type 2 diabetes shares causal factors with cardiovascular disease, particularly CHD. For example, lifestyle, especially physical activity, is important for preventing Type 2 diabetes or delaying its onset [4].
A number of prospective cohort studies [5, 6, 7, 8, 9, 10, 11, 12, 13, 14] have reported that greater physical activity or energy expenditure is associated with a substantial reduction in the risk of Type 2 diabetes. The majority of these studies have examined the relationship between specific physical activities (such as walking, occupational and leisure-time physical activity, and more vigorous activities) and the risk of Type 2 diabetes; however, the potential effect of different types of daily life physical activities remains to be determined. These activities represent the accumulation of complex behaviours in daily life and few middle-aged individuals engage in physical training or physical activity at their jobs or during leisure time. It is therefore important to further examine whether overall physical activity in daily life contributes to a reduction of the risk of diabetes. This study prospectively examined the relationship between daily life activities (expressed in terms of energy expenditure) and the incidence of IFG and Type 2 diabetes (diagnosed according to the criteria of the American Diabetes Association for epidemiological studies [15]), in normoglycaemic Japanese male office workers over a 7-year observation period.
Subjects and methods
Study cohort
To evaluate the potential association between daily life activity and the development of IFG or Type 2 diabetes, a survey of the incidence of IFG or Type 2 diabetes was carried out between 1994 and 2001 in Japanese men who were office workers at one of Japan’s biggest building contractors. All Japanese male office workers aged 35 to 59 years in May 1994 were invited to participate in annual health examinations (n=3694); the participation rate was 99.6% (n=3681). The Industrial Safety and Health Law in Japan requires the employer to conduct annual health examinations of all employees. The employee data, which are anonymous, are available for research with the approval of the employer. An institutional review committee approved this study, and all subjects gave their informed consent to participate.
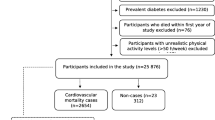
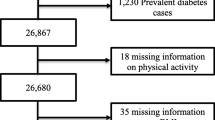
Of the 3681 potential participants, 46 (1.2%) did not return the activity record for daily life activities or did not complete the record. Of the other subjects, 647 (17.8%) were excluded: 172 (4.7%) had IFG, 276 (7.6%) had Type 2 diabetes, 247 (6.8%) were taking anti-hypertensive medication and 28 (0.8%) had a past history of CHD or stroke. Thus, the baseline population consisted of 2988 men. Since we also excluded 64 men who did not participate in consecutive annual health examinations, the final study population for analysis consisted of 2924 men. Men with IFG or Type 2 diabetes identified during consecutive surveys through May 2001 were classified as having these conditions. To determine the incidence of Type 2 diabetes, incident cases of IFG were followed-up and were considered Type 2 diabetes if they reached that endpoint during the study. In total, 39 participants who started taking medication for diabetes during the observation period were considered to be incident cases of Type 2 diabetes. Owing to the age range of the study population, all cases of IFG or Type 2 diabetes were diagnosed after 35 years of age.
Study design
Fasting plasma glucose levels were measured at annual health examinations performed from 1994 to 2001. The participants were asked to fast for at least 8 h and to avoid smoking and heavy physical activity for more than 2 h before the examinations. Blood samples were drawn from an antecubital vein, and glucose was measured with the hexokinase–glucose dehydrogenase method [16, 17]. Quality control of the laboratory was internal, and the coefficients of variation between and within assays for plasma glucose were no more than 3% during the study period. Normal fasting glucose, IFG and Type 2 diabetes were defined according to the criteria of the American Diabetes Association [15]. Fasting glucose levels were used to make a diagnosis since not every subject underwent an OGTT. Normal fasting glucose was defined as a fasting plasma glucose level of less than 6.1 mmol/l. IFG was defined as a fasting plasma glucose level of at least 6.1 mmol/l but less than 7.0 mmol/l. Type 2 diabetes was defined as a fasting plasma glucose level of 7.0 mmol/l or higher or treatment with hypoglycaemic medications.
Annual health examination items at study entry included medical history, physical examination, anthropometric measurements, blood pressure measurement, biochemical measurements and an activity record for the assessment of daily energy expenditure, as well as a questionnaire on health-related behaviour, such as physical exercise, smoking and alcohol consumption. Medical history and history of use of prescription drugs were assessed by the examining physicians. A family history of diabetes was defined as having a mother, father, sister and/or brother with diagnosed diabetes. Body mass index (kg/m2) was used as a measure of overall obesity. After a 5-min rest in a quiet room, systolic and diastolic blood pressures were measured using a standard mercury sphygmomanometer, placing the cuff on the right arm. The levels of serum total cholesterol, HDL cholesterol and triglycerides were determined using standard laboratory procedures [16, 17]. A 1-day activity record during an ordinary weekday was designed to estimate energy expenditure. The activity record for 1 day was divided into 96 periods of 15 min each [18]. We predefined 20 typical daily weekday physical activities in this population (Table 1) and participants were asked to write the categorical values that best reflected the dominant activity of each 15-min period in the space provided. The approximate energy cost for each category (in kcal·kg–1·15 min–1) for Japanese men was used to calculate the daily energy expenditure for each individual [19]. If an activity could not be assigned to one of the predefined categories, the subjects were asked to describe the activity in more detail. Daily energy expenditure was calculated by multiplying the amount of time spent on specific daily physical activities by the energy cost per physical activity and the weight of the individual in kg. Participants were also asked about the type of physical exercise and the amount of time spent per week on physical exercise. Physical exercise was defined as participation in any physical activity, such as jogging, bicycling, swimming or tennis, that was performed long enough to cause sweating. Weekly energy expenditure on physical exercise was calculated by multiplying the amount of time spent on specific exercises by the energy cost per exercise and the weight of the individual in kg. The questionnaire also asked about cigarette smoking habits (never, past or current smoker); past or current smokers were asked to specify the number of cigarettes smoked per day and the number of years they had been smoking. The questions relating to alcohol intake included items about the type of alcoholic beverage, the frequency of alcohol consumption per week and the usual amount consumed daily. Weekly alcohol intake was calculated and then converted to daily alcohol consumption (grams of ethanol per day) using standard Japanese tables.
Statistical analysis
Data are reported as means ± SD except when the distribution was strongly skewed, in which case medians and interquartile ranges are given. One-way analysis of variance and the chi square test were used to analyse the statistical differences in baseline characteristics between study participants according to quartile of daily energy expenditure. Categories of daily life energy expenditure were defined by the following quartiles: <33.1 kcal·kg–1·day–1, 33.1–36.7 kcal·kg–1·day–1, 36.8–40.3 kcal·kg–1·day–1 and ≥40.4 kcal·kg–1·day–1. For each participant, person-years of follow-up were calculated from the date of enrolment to either the date of the last follow-up or the date of the follow-up at which IFG or Type 2 diabetes was detected, whichever came first. Follow-up time included 92.8% of the total potential person-years of follow-up. Cox’s proportional hazards models were used to evaluate the association between daily energy expenditure level and the development of IFG or Type 2 diabetes. Data were adjusted for age, family history of diabetes, alcohol consumption, cigarette smoking, BMI, weekly energy expenditure on physical exercise, systolic blood pressure, HDL cholesterol and triglycerides at study entry. The following potential confounding factors were treated as categorical variables: age, BMI, systolic blood pressure, HDL cholesterol, triglycerides (graded from 1 through 5 [first through fifth quintiles]), family history of diabetes (no or yes), alcohol consumption (graded as 1 [none] or as grade 2 [quartile 1] to grade 5 [quartile 4] for drinkers), cigarette smoking (graded as 1 [none] or as grade 2 [quartile 1] to grade 5 [quartile 4] for current smokers) and weekly energy expenditure on physical exercise (graded as 1 [none] or as grade 2 [tertile 1 or 2] or grade 3 [tertile 3] for men engaging in regular physical exercise). The linear trends of risks were evaluated by entering indicators for each category of exposure. The interactions between daily life energy expenditure and each of the potential risk factors were tested by introducing product terms to models with the original variables.
Data were analysed using SPSS statistical software (SPSS, Chicago, Ill., USA). All reported p values are two-tailed, and those less than 0.05 were considered statistically significant.
Results
Table 2 shows the baseline characteristics of the study sample divided into quartiles according to daily energy expenditure. Men in the lowest quartile of daily energy expenditure were the oldest. BMI, systolic and diastolic blood pressures, and the levels of total cholesterol, triglycerides and fasting plasma glucose decreased with increasing daily energy expenditure. In contrast, HDL cholesterol level, weekly energy expenditure on physical exercise and the percentage of those who exercised at least once a week increased with increasing daily energy expenditure. Family history of diabetes, alcohol consumption and cigarette smoking did not differ significantly across quartiles of daily energy expenditure.
During the 7 years of follow-up, representing 18,102 person-years, 280 men developed IFG (Table 3). The results were controlled for age, family history of diabetes, alcohol consumption, cigarette smoking, BMI, weekly energy expenditure on physical exercise, systolic blood pressure, HDL cholesterol and triglycerides at study entry. After adjustment, the relative risks for IFG across quartiles of daily life energy expenditure (lowest to highest) were 1.00, 0.71, 0.67 and 0.40 (p<0.001 for trend). Type 2 diabetes was diagnosed in 168 men during 7-years of follow-up (representing 18 416 person-years). The corresponding multivariate-adjusted relative risks for Type 2 diabetes were 1.00, 0.76, 0.70 and 0.41 (p=0.001 for trend). In further analyses, IFG and Type 2 diabetes were combined on the assumption that the two conditions develop via similar mechanisms.
Table 4 shows the risk of developing IFG or Type 2 diabetes according to selected daily life activities. The age-adjusted relative risk of IFG or Type 2 diabetes progressively decreased with increasing energy expenditure on occupational physical activity, brisk walking, riding on vehicles (standing position) to and from work and other physical activities (p<0.001 for trend for all). After additional adjustment for the potential confounders of diabetes, riding on vehicles (standing position) to and from work and other physical activities showed a significant linear trend (p=0.026 and p=0.003 for trend respectively).
Results of stratified analyses by the presence or absence of a risk factor for diabetes (age, family history of diabetes, alcohol use, cigarette smoking, obesity and regular physical exercise) are shown in Table 5. After adjustment for various potential confounders for diabetes, the risk of developing IFG or Type 2 diabetes was inversely related to the daily energy expenditure, both in men at low risk of diabetes and those at high risk. The results of tests for interaction between daily energy expenditure and these risk factors in terms of developing IFG or Type 2 diabetes were not statistically significant.
Discussion
Our results showed that physical activity in daily life, expressed in terms of daily energy expenditure, was inversely associated with the risk of developing IFG or Type 2 diabetes even after adjustment for potential confounders of diabetes. As regards the type of daily physical activity, occupational physical activity, brisk walking, riding on vehicles (standing position) to and from work, and other physical activities were associated with a substantial reduction in risk of developing IFG or Type 2 diabetes. These findings indicate that increasing daily life activity, especially through the aforementioned activities, is an effective way of reducing the risk of developing IFG or Type 2 diabetes in Japanese male office workers. Conversely, walking or cycling, when analysed together, was not associated with a decreased risk of developing IFG or Type 2 diabetes. Because few men engaged in cycling in this population, energy expenditure on walking, including walking at normal speed and brisk walking, was higher than that on cycling. When analysed on its own, the results indicated that brisk walking (i.e. walking pace) is an important factor in the prevention of IFG or Type 2 diabetes. However, on adjustment for potential confounders of diabetes, the inverse association between each daily physical activity and the risk of developing IFG or Type 2 diabetes was substantially attenuated. Being overweight or obese has been shown to be an important risk factor for Type 2 diabetes [20, 21]. In this study, BMI differed significantly between the subgroups of energy expenditure for each physical activity (p<0.001 for all), and men who spent less energy on each daily physical activity had the higher BMI value. Daily life activities may indirectly reduce the risk of IFG or Type 2 diabetes through decreased body weight. Overweight and obese people are less likely to engage in physical activity, and physical activity facilitates weight loss and weight maintenance [22].
Stratified analyses by the presence or absence of different risk factors showed the protective effect of increased daily life activity both in men at low risk of diabetes and those at high risk. However, daily life activity had no significant effect on the risk of developing IFG or Type 2 diabetes in subjects with a family history of diabetes or in those who currently abstained from alcohol. This lack of effect may be the result of the small number of subjects in these subgroups. In addition, Japanese individuals have a higher prevalence of polymorphisms in a number of genes encoding proteins that are thought to play key roles in lipid and glucose metabolism, including the β3-adrenergic receptor, the peroxisome proliferator-activated receptor-γ and calpain-10 genes [23]. Thus, the thrifty genotype characteristics may be confounding factors.
Our results are consistent with the concept that greater physical activity substantially reduces the risk of developing diabetes [5, 6, 7, 8, 9, 10, 11, 12, 13, 14]. Although the underlying mechanism of this effect remains unclear, the finding that an increase in daily life activity is associated with a lower risk of diabetes is biologically plausible. Physical activity independently increases both insulin-mediated and non-insulin-mediated glucose metabolism [24]. The increase in insulin sensitivity is the result of an increase in the number and activity of glucose transporters (especially the GLUT4 isoform), which are stimulated by muscle contraction [25, 26]. Insulin-stimulated glycogen synthesis is also increased in active muscles [27]. Furthermore, fat oxidation (whether from circulating free fatty acids or muscle triglycerides) is enhanced during activity of any intensity [28], and physical activity results in a reduced adipose tissue mass and preserves or increases the lean body mass [22], which also leads to an increase in insulin sensitivity. These phenomena suggest that daily life activity of any intensity has the potential to favourably affect insulin sensitivity or to prevent IFG or Type 2 diabetes.
Our study was subject to several limitations. Firstly, a 1-day activity record during an ordinary weekday was used to estimate overall energy expenditure. This may have led to inaccuracies in exposure measures and may have resulted in a biased estimate of the association between daily energy expenditure and the risk of diabetes. In this study, there was a clear dose-response relationship between daily energy expenditure and biological markers of physical activity such as HDL cholesterol level (r=0.301, p<0.001) and triglyceride level (r=−0.319, p<0.001). In addition, in Japan, an employee often stays at the same job until retirement. Thus, physical activity in daily life may be a consistent and reliable indicator of an individual’s physical activity status throughout his adult life.
Secondly, participants in this study, particularly those in the older age groups, might not be typical of the general population. Men with a plasma glucose level above the threshold values for IFG or Type 2 diabetes, or who reported taking drugs for hypertension or a history of CHD or stroke during the initial examination were excluded. Because hypertension is a recognised risk factor for diabetes [29, 30], exclusion of hypertensive persons would bias the study towards a particularly healthy study population with a low risk of diabetes. The selection at study entry of men with rigorously normal fasting plasma glucose levels could have affected the observations. Furthermore, all the participants in this study were white-collar workers, not working a shift pattern, and three-fifths of the participants were architects or research workers. The percentage of those who had 13 years of education was about 95%. As the cohort studied was a restricted social class group of white-collar workers, the results cannot be extended to a national population.
Finally, only selected variables were assessed as confounding factors for diabetes incidence. We did not assess participants’ visceral adiposity (WHR), fasting insulin level or dietary habits. The central pattern of weight distribution (as indicated by an increased WHR) is associated with a higher frequency of insulin resistance than the peripheral pattern of distribution, and individuals with the central distribution pattern are more likely to have glucose intolerance and hyperinsulinaemia resulting from insulin resistance [31, 32]. Dietary lipids, fibre or carbohydrates may influence fasting insulin levels [33, 34], and diets with a high glycaemic load that are low cereal fibre may be associated with the risk of Type 2 diabetes [35]. Furthermore, an OGTT was not performed at baseline or during follow-up in this study. Thus, some cases of asymptomatic diabetes at baseline and during follow-up may have been included. Therefore, visceral adiposity (WHR), fasting insulin levels, dietary habits and an OGTT test should be included in future studies.
Despite these potential limitations, our findings support the conclusion that physical activity in daily life is inversely associated with the risk of developing IFG or Type 2 diabetes. Public health recommendations for an increase in daily life activity may help to reduce the development of IFG or Type 2 diabetes.
References
King H, Aubert RE, Herman WH (1998) Global burden of diabetes, 1995-2025: prevalence, numerical estimates, and projections. Diabetes Care 21:1414–1431
Barrett-Connor E (1989) Epidemiology, obesity, and non-insulin-dependent diabetes mellitus. Epidemiol Rev 11:172–181
Morris RD, Rimm DL, Hartz AJ, Kalkhoff RK, Rimm AA (1989) Obesity and heredity in the etiology of non-insulin-dependent diabetes mellitus in 32 662 adult white women. Am J Epidemiol 130:112–121
Tuomilehto J, Tuomilehto-Wolf E, Zimmet P, Alberti KG, Knowler WC (1997) Primary prevention in diabetes mellitus. In: Alberti KG, Zimmet P, DeFronzo RA, Keen H (eds) International textbook of diabetes mellitus, 2nd edn. Wiley, Chichester, UK, pp 1799–1827
Helmrich SP, Ragland DR, Leung RW, Paffenbarger RS Jr (1991) Physical activity and reduced occurrence of non-insulin-dependent diabetes mellitus. N Engl J Med 325:147–152
Manson JE, Rimm EB, Stampfer MJ et al. (1991) Physical activity and incidence of non-insulin-dependent diabetes mellitus in women. Lancet 338:774–778
Manson JE, Nathan DM, Krolewski AS, Stampfer MJ, Willett WC, Hennekens CH (1992) A prospective study of exercise and incidence of diabetes among US male physicians. JAMA 268:63–67
Burchfiel CM, Sharp DS, Curb JD et al. (1995) Physical activity and incidence of diabetes: the Honolulu Heart Program. Am J Epidemiol 141:360–368
Perry IJ, Wannamethee SG, Walker MK, Thomson AG, Whincup PH, Shaper AG (1995) Prospective study of risk factors for development of non-insulin dependent diabetes in middle aged British men. BMJ 310:560–564
Lynch J, Helmrich SP, Lakka TA et al. (1996) Moderately intense physical activities and high levels of cardiorespiratory fitness reduce the risk of non-insulin-dependent diabetes mellitus in middle-aged men. Arch Intern Med 156:1307–1314
Haapanen N, Miilunpalo S, Vuori I, Oja P, Pasanen M (1997) Association of leisure time physical activity with the risk of coronary heart disease, hypertension and diabetes in middle-aged men and women. Int J Epidemiol 26:739–747
Hu FB, Sigal RJ, Rich-Edwards JW et al. (1999) Walking compared with vigorous physical activity and risk of type 2 diabetes in women: a prospective study. JAMA 282:1433–1439
Wannamethee SG, Shaper AG, Alberti KG (2000) Physical activity, metabolic factors, and the incidence of coronary heart disease and type 2 diabetes. Arch Intern Med 160:2108–2116
Hu G, Qiao Q, Silventoinen K et al. (2003) Occupational, commuting, and leisure-time physical activity in relation to risk for Type 2 diabetes in middle-aged Finnish men and women. Diabetologia 46:322–329
The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus (1997) Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 20:1183–1197
Nakanishi N, Yoshida H, Matsuo Y, Suzuki K, Tatara K (2002) White blood-cell count and the risk of impaired fasting glucose or Type II diabetes in middle-aged Japanese men. Diabetologia 45:42–48
Nakanishi N, Suzuki K, Tatara K (2003) Alcohol consumption and risk for development of impaired fasting glucose or type 2 diabetes in middle-aged Japanese men. Diabetes Care 26:48–54
Bouchard C, Tremblay A, Leblanc C, Lortie G, Savard R, Theriault G (1983) A method to assess energy expenditure in children and adults. Am J Clin Nutr 37:461–467
Health Promotion and Nutrition Division, Health Service Bureau, Ministry of Health and Welfare (1989) Recommended Dietary Allowance for the Japanese, 4th edn [in Japanese]. Dai-Ichi Shuppan, Tokyo [in Japanese]
Chan JM, Rimm EB, Colditz GA, Stampfer MJ, Willett WC (1994) Obesity, fat distribution, and weight gain as risk factors for clinical diabetes in men. Diabetes Care 17:961–969
Colditz GA, Willett WC, Rotnitzky A, Manson JE (1995) Weight gain as a risk factor for clinical diabetes mellitus in women. Ann Intern Med 122:481–486
Blair SN (1993) Evidence for success of exercise in weight loss and control. Ann Intern Med 119:702–706
Kawamori R (2002) Diabetes trends in Japan. Diabetes Metab Res Rev 18 [Suppl 3]:S9–S13
Goodyear LJ, Hirshman MF, Horton ES (1991) Exercise-induced translocation of skeletal muscle glucose transporters. Am J Physiol 261:E795–E799
Brozinick JT Jr, Etgen GJ Jr, Yaspelkis BB III, Ivy JL (1992) Contraction-activated glucose uptake is normal in insulin-resistant muscle of the obese Zucker rat. J Appl Physiol 73:382–387
Henriksson J (1995) Influence of exercise on insulin sensitivity. J Cardiovasc Risk 2:303–309
Perseghin G, Price TB, Petersen KF et al. (1996) Increased glucose transport-phosphorylation and muscle glycogen synthesis after exercise training in insulin-resistant subjects. N Engl J Med 335:1357–1362
Romijn JA, Coyle EF, Sidossis LS et al. (1993) Regulation of endogenous fat and carbohydrate metabolism in relation to exercise intensity and duration. Am J Physiol 265:E380–E391
Stolk RP, Splunder IP van, Schouten JS, Witteman JC, Hofman A, Grobbee DE (1993) High blood pressure and the incidence of non-insulin dependent diabetes mellitus: findings in a 11.5 year follow-up study in The Netherlands. Eur J Epidemiol 9:134–139
Morales PA, Mitchell BD, Valdez RA, Hazuda HP, Stern MP, Haffner SM (1993) Incidence of NIDDM and impaired glucose tolerance in hypertensive subjects. The San Antonio Heart Study. Diabetes 42:154–161
Krotkiewski M, Bjorntorp P, Sjostrom L, Smith U (1983) Impact of obesity on metabolism in men and women. Importance of regional adipose tissue distribution. J Clin Invest 72:1150–1162
Pouliot MC, Després JP, Nadeau A et al. (1992) Visceral obesity in men. Associations with glucose tolerance, plasma insulin, and lipoprotein levels. Diabetes 41:826–834
Anderson JW, Gustafson NS, Bryart CA, Tietyen-Clark J (1987) Dietary fiber and diabetes. J Am Diet Assoc 87:1189–1197
Mayer EJ, Newman B, Quesenberry CP Jr, Selby JV (1993) Usual dietary fat intake and insulin concentrations in healthy women twins. Diabetes Care 16:1459–1469
Salmeron J, Manson JE, Stampfer MJ, Colditz GA, Wing AL, Willett WC (1997) Dietary fiber, glycemic load, and risk of non-insulin-dependent diabetes mellitus in women. JAMA 277:472–477
Acknowledgements
This study was supported in part by Grants-in-Aid from the Japanese Arteriosclerosis Prevention Fund (JAPF), Tokyo, Japan and the Smoking Research Foundation, Tokyo, Japan.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nakanishi, N., Takatorige, T. & Suzuki, K. Daily life activity and risk of developing impaired fasting glucose or Type 2 diabetes in middle-aged Japanese men. Diabetologia 47, 1768–1775 (2004). https://doi.org/10.1007/s00125-004-1528-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-004-1528-y