
Abstract
Purpose
Management practices associated with war-related amputations in countries at war may be different from the recommendations of occidental Health Force Services due to the high numbers of wounded persons to treat in precarious conditions. This observational retrospective study documents the current management of local lower extremity amputees in Afghanistan. Surgical practices, with or without delayed primary closure (DPC), and prosthetic rehabilitation issues are analyzed.
Methods
This retrospective study was conducted in the National Military Hospital (NMH) of Kabul from May 2011 to November 2011. Fifty-four Afghan patients who underwent a lower extremity combat-related amputation were included. Ten of them sustained a bilateral amputation.
Results
Injuries were caused by improvised explosive devices (IEDs) or mines in 48 cases, bullets in three cases, and exploding shell fragments in three cases. Of the 64 amputations studied, 46 were open length preserving amputations and primary closure (PC) was applied in 18 cases. Patients were reviewed with a mean follow-up of 5.4 months (range 1–28 months). In the DPC group, secondary closure was performed with a mean time of 18.7 days (range 4–45 days) from injury. The proportion of infectious complications seemed to be higher in the PC group (5/18) than in the DPC group (3/46), but it was only a statistical trend (p = 0.1). Forty-three patients were not prosthetic fitted at the last follow-up.
Conclusion
This study supports the surgical strategy of a two-stage procedure for lower limb amputations in countries at war, but underlines the problems of late secondary closure and prosthetic fitting related to decreased sanitary conditions.
Similar content being viewed by others

Introduction
Extremities remain the most common site of combat-related injuries in the current Afghanistan war [1]. Improvised explosive devices (IEDs) have become the main threat to Afghan National Army (ANA) troops, with a special involvement of the lower extremity [2–4]. In these complex blast injuries, amputations are often bilateral, proximal, and highly contaminated [3–5]. Conventional war weapons are also widely used, with mangled extremity injuries caused by fragments or bullets. Despite advances in both vascular and orthopedic reconstructive surgery, limb salvage is not always possible or suitable, and primary amputation is often required [6].
In the military context, the current rule is to amputate as conservatively as possible in viable tissues with delayed primary closure (DPC). The final level of amputation and definitive treatment takes place after evacuation in a stable environment [6, 7]. A primary “open length preserving amputation” is recommended at the lowest possible level of bone [8]. The soft tissues distally should be preserved to be used in the subsequent closure of the amputation stump [6]. However, surgical practices associated with amputations in countries at war may be different from those of occidental Health Force Services, and primary closure (PC) of stumps still seems to be performed [9]. Several factors can explain these differences: a high number of wounded persons with amputation to treat; the lack of means of transportation, equipment, or medical supplies [9–11]. Furthermore, access to facilities for rehabilitation and prosthetic fitting is challenging in precarious conditions.
The purpose of this study was to investigate the current surgical management of combat-related lower extremity amputations in Afghan patients, especially concerning the application of the DPC concept. Access to early prosthetic rehabilitation was also analyzed.
Methods
An observational retrospective study was conducted in the orthopedic surgery department of the National Military Hospital (NMH) of Kabul between May 1, 2011 and November 1, 2011 by two external observers (LM and AM). All patients hospitalized after a combat-related lower extremity amputation were included during this period. Patients were soldiers of the ANA or civilians transferred from other medical facilities all over the country for definitive treatment and rehabilitation.
Most of the patients were wounded outside of the Kabul province, and were first treated in an Afghan regional hospital or International Security Assistance Forces (ISAF) medical facilities. Initial management consisted in the debridement of traumatic amputations or primary amputation for unsalvageable mangled extremities. Patients who received early secondary amputations after evacuation from the battlefield were also included, as well as patients readmitted for complications after amputation. The concept of DPC was applied for patients treated in ANA or ISAF medical facilities, but some PCs were performed in civilian hospitals. In cases of DPC, bulky absorbent dressings were changed every 2 or 3 days in the ward until the wound was clean and ready for closure. The closure of transtibial or femoral amputations was preceded by a limited soft-tissue and bone re-cutting, and closure of knee disarticulations consisted in a Gritti procedure (Fig. 1).

Example of two-stage amputation: primary open knee disarticulation; secondary closure by a Gritti procedure
Medical records and radiographs were reviewed to confirm demographic, injury, and amputation information. The following data were extracted for analysis: mechanism of injury, level of amputation, associated injuries, primary or secondary closure, and time from injury to DPC. Because of a high percentage of bilateral amputees, with various treatments according to the side considered, the global number of amputations was considered for clinical assessment. Amputations were categorized into two groups based on their initial management: PC group and DPC group. Amputation levels were classified as hindquarter (HQA) when at the hip, above knee amputation (AKA) including knee disarticulation, below knee amputation (BKA), and Syme when at the hind-foot level.
Physical and radiological examinations were performed to investigate complications, including infection or other stump problems. During this period, laboratory facilities were limited, and microbiology assessment was often unavailable. A deep soft-tissue infection was defined as any infection that was not successfully treated by empiric antibiotics or local care and required revision surgery [12]. Osteomyelitis was defined as a deep infection with osteolysis or periosteal reaction on X-rays. Functional assessment was limited to the use of temporary or definitive prosthesis, crutches, or wheelchair.
Statistical analysis was performed with Epi-Info version 6.04 (Centers for Disease Control and Prevention, CDC, USA, update October 2000) to assess for differences across groups. Dichotomous variables were compared using the Chi-square test or Fisher’s exact test for the comparison of proportions when numbers were below 5. A p-value of ≤0.05 was considered significant.
Results
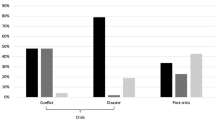
Over the period reviewed, 54 lower extremity amputees were admitted and treated in the NMH. All of the patients were men. The average age at the time of injury was 23.3 years (range 17–40 years). Thirty-one patients (57 %) were wounded in the southern provinces of Helmand and Kandahar. Most of the others were transferred from eastern provinces or Pakistan (Fig. 2).

Provinces of injury and initial management (*East provinces include Kapisa, Logar, Nuristan, Paktiya)
Injury patterns
Injuries were caused by IEDs or mines in 48 cases, bullets in three cases, and exploding shell fragments in three cases.
Forty-four patients sustained a unilateral lower limb amputation, and ten patients underwent a bilateral amputation. Thirty-two patients had a total of 46 associated injuries: 19 patients had one associated injury, 12 patients had two associated injuries, and one patient had three associated injuries. Multiple soft-tissue wounds and lower extremity fractures were predominant (Table 1).
Among the 64 amputations studied, there was one HQA, 28 AKA, 34 BKA, and one Syme amputation. Distributions of traumatic amputations and trauma-related amputations (primary or secondary) among different level amputation groups were equivalent (Table 2). The three secondary amputations were performed 3–30 days from injury after failure of conservative treatment. Bilateral AKA/traumatic amputation was the most common presentation among bilateral amputees (Table 3).
Clinical assessment (64 amputations)
There were 46 amputations in the DPC group and 18 amputations in the PC group. The average follow-up after injury was 5.4 months (range 1–28 months).
In the DPC group, an iterative surgical debridement was required prior to closure in 12 of the 46 cases. Secondary closure was performed with a mean time of 18.7 days (range 4–45 days) from injury. At the last follow-up, three infectious complications were reported: one superficial soft-tissue infection in the postoperative period and two cases of tibial osteomyelitis that required revision surgery several months after BKA.
In the PC group, five infectious complications were reported in the postoperative period: four deep soft-tissue infections that required re-amputation at a more proximal level, and one superficial infection treated by the removal of skin stitches. The proportion of infectious complications seemed to be higher in the PC group (5/18) than in the DPC group (3/46), but it was only a statistical trend (p = 0.1).
Functional assessment (54 patients)
Only 11 patients were prosthetic fitted at the last follow-up. Four of them had no problem with their prosthesis, but seven were hospitalized for late complications impairing prosthesis use (bone spurs in two cases, knee stiffness in two cases, failure of myodesis in three cases).
Over the 43 non-prosthetic fitted patients, the lack of prosthetic rehabilitation was due to a short-term follow-up (mean 2.3 months, range 1–8 months) in 37 cases. One case was the Syme amputation for which prosthesis was not necessary. Other cases were four proximal AKA in two bilateral amputees who failed to succeed in prosthetic fitting more than one year after injury, and who still used a wheelchair.
Discussion
Most of the patients of this cohort were injured in Southern Afghanistan, where IED attacks have become increasingly frequent during the last several years [2, 3]. Injuries caused by IED are specific, with multiple amputations associated with greater injury burden and mortality [2–4]. Furthermore, many civilian patients were injured by land mines or unexploded ordnances that pose a significant public health risk in Afghanistan [13]. The optimal management of theses severe injuries often required complex reconstructive procedures and sophisticated prosthetic rehabilitation that are seldom available in countries at war.
According to the International Committee of the Red Cross (ICRC), war wounds need only two operations if managed properly. The first operation is a wound excision or amputation upon admission and the second the delayed primary suture after 5 days, because this is the predicted time when the bacterial count in the wound is at its lowest. If the wounds are not clean enough after 5 days, then more extensive wound excision or higher amputation should take place, finally followed by a secondary closure [14, 15]. The present guidelines on amputations in the field hospital are based on this concept of a two-stage procedure: debridement and DPC (Table 4) [6, 7]. Health Force Services of highly developed countries, with their field medical facilities and their ability to rapidly evacuate patients to trauma centers, can perform these tasks in a fairly easy manner [9].
In Afghanistan, the large number of casualties and the lack of means of evacuation, hospitals, equipment, or medical supplies make sequential surgical procedures difficult to apply for local casualties. Ensuring fast and successful treatment is often needed in order to do the best for most surgical procedures [9]. That explains why some patients managed in civilian regional hospitals underwent amputation with PC. According to Muminagic [9], the primary suture of war amputation wound can be successful under certain conditions: when performed in a hospital, by an educated team, within 6 h from the injury, after a fitted pre-hospital management in the battlefield. Over the 528 patients treated in Muminagic’s cohort [9], the results of primary suture were better on upper extremity injuries (61.9 % successful) than on lower extremity injuries (48.8 % successful). The higher rate of infectious complications after PC observed in this study confirms that this one-stage management is risky for lower limb amputations, and should not be recommended even under deteriorated conditions due to the context of war. At the present time, the ANA Health Force Services send experienced surgical teams to regional hospitals to help and teach local surgeons in the management of war casualties.
Most of the patients in this cohort received sequential management according to the rules of modern war surgery. However, the mean time of 18.7 days for secondary closure underlines difficulties in achieving a two-stage amputation in these circumstances. Only four patients underwent DPC within 7 days after injury. In the other cases, late DPC could be explained by several factors. First, blast injuries due to IEDs or land mines were highly contaminated and required serial debridements prior to secondary closure [5]. In addition, evacuations from the battlefield may have been delayed by difficulties concerning inter-hospital transport in a combat environment, especially for the patients coming from southern or western provinces. The medical evacuation (MEDEVAC) system in the ANA is growing fast, but most of the patients are still evacuated by road due to the lack of air transportation means. While coalition troops usually stay in deployed hospitals for a few hours before evacuation out of theater, the time spent by local troops or civilians is longer [16]. Thus, when patients arrived in the NMH, wounds may have been contaminated by the nosocomial transmission of pathogens along the evacuation chain [16, 17]. Finally, environmental contamination of the stumps might be explained by iterative dressing exchanges in the ward due to an important operative schedule. All open wounds were dressed by saline-soaked gauze and crepe bandage, as per current recommendations [16, 18]. Topical negative pressure wound therapy (TNPWT) should have been useful to limit environmental contamination and reduce the time from admission to secondary closure, but it was not available in the NMH [19] (Fig. 3).

Bilateral amputee with perineal lesions wounded by an improvised explosive device (IED) and treated by topical negative pressure wound therapy (TNPWT). TNPWT has multiple advantages in this case (better drainage of cavitary wounds, decrease of muscle edema, protection against environmental and anal contaminations, fewer dressing exchanges), but cannot be performed in precarious conditions
Despite a short-term follow-up, this study underlines that the management of amputees in Afghanistan is hindered by the lack of facilities for prosthetic rehabilitation. Early prosthetic fitting is not possible in the NMH, and patients have to be transferred to ICRC limb-fitting centers (one center is located in Kabul) or to hospitals in border countries. At the present time, efforts are being made by the ANA Health Force Services to build a prosthetic rehabilitation center in annex to the NMH. Furthermore, this cohort is characterized by numerous bilateral above knee amputees for whom prosthetic fitting is almost impossible in this context. Even in advanced rehabilitation centers of highly developed countries, prosthetic fitting of bilateral AKA is challenging, and requires sophisticated technology that is not available in this part of the world. The wheelchair is the only way for these young patients who become totally dependent on their family. In addition to being accessible, prosthetics (or wheelchairs) must be adapted to the living conditions of a mostly mountain dweller amputee population in Afghanistan, i.e., cold, humid, and steep roads [11].
This study has several limitations. First, this is a retrospective analysis and carries shortcomings inherent to the study design. Although injuries were consistently similar, initial management was not standardized and varied according to the patient’s origin. Second, our analysis of infectious complications is limited by the absence of microbiology assessment. Swabs of all open stumps at the time of patient arrival in the NMH would have been useful for the documentation of nosocomial wound contamination. Finally, our findings are focused on stump management and prosthetic fitting, but pain management and psychosocial impacts of lower limb amputations are not analyzed.
Conclusion
This study underlines the problem of surgical management and prosthetic fitting of lower limb amputees in Afghanistan. Despite a limited methodology, our results support the surgical strategy of a two-stage procedure with open length amputation and DPC. However, in these circumstances, the time from injury to secondary closure may be delayed by the nosocomial colonization of open stumps due to the difficulties of MEDEVAC from the battlefield, high numbers of patients to treat, limited access to the operating theater, and by the lack of TNPWT or other medical supplies. Afterwards, prosthetic fitting remains difficult, especially for the numerous victims of IEDs with bilateral AKA for whom social and professional reintegration is jeopardized. Improvement in the MEDEVAC system and construction of a prosthetic rehabilitation center are the current priorities of the ANA Health Force Services.
References
Owens BD, Kragh JF Jr, Wenke JC, Macaitis J, Wade CE, Holcomb JB. Combat wounds in operation Iraqi Freedom and operation Enduring Freedom. J Trauma. 2008;64:295–9.
Ramasamy A, Hill AM, Clasper JC. Improvised explosive devices: pathophysiology, injury profiles and current medical management. J R Army Med Corps. 2012;155:265–72.
Krueger CA, Wenke JC, Ficke JR. Ten years at war: comprehensive analysis of amputation trends. J Trauma Acute Care Surg. 2012;73(Suppl 5):S438–44.
Brown KV, Guthrie HC, Ramasamy A, Kendrew JM, Clasper J. Modern military surgery: lessons from Iraq and Afghanistan. J Bone Joint Surg Br. 2012;94:536–43.
Evriviades D, Jeffery S, Cubison T, Lawton G, Gill M, Mortiboy D. Shaping the military wound: issues surrounding the reconstruction of injured servicemen at the Royal Centre for Defence Medicine. Philos Trans R Soc Lond B Biol Sci. 2011;366:219–30.
Rigal S. Extremity amputation: how to face challenging problems in a precarious environment. Int Orthop. 2012;36:1989–93. doi:10.1007/s00264-012-1548-z.
Clasper J; Lower Limb Trauma Working Group. Amputations of the lower limb: a multidisciplinary consensus. J R Army Med Corps. 2007;153:172–4.
Chapter 25: Amputations. In: Szul AC, Davis LB (eds) Emergency war surgery: third United States revision. Borden Institute, Walter Reed Army Medical Center; 2004. p. 25.1–25.8.
Muminagic SN. Primary suture of amputation wound: pro et contra. Med Arh. 2011;65(3):188–90.
Tintle SM, Keeling JJ, Shawen SB, Forsberg JA, Potter BK. Traumatic and trauma-related amputations: part I: general principles and lower-extremity amputations. J Bone Joint Surg Am. 2010;92:2852–68.
Bisseriex H, Rogez D, Thomas M, Truffaut S, Compere S, Mercier H, Dochez F, Lapeyre E, Thefenne L. Amputation in low-income countries: particularities in epidemiological features and management practices. Med Trop (Mars). 2011;71:565–71.
Huh J, Stinner DJ, Burns TC, Hsu JR; Late Amputation Study Team. Infectious complications and soft tissue injury contribute to late amputation after severe lower extremity trauma. J Trauma. 2011;71(Suppl 1):S47–51.
Bilukha OO, Brennan M, Woodruff BA. Death and injury from landmines and unexploded ordnance in Afghanistan. JAMA. 2003;290:650–3.
Coupland RM. Technical aspects of war wound excision. Br J Surg. 1989;76:663–7.
Korver AJH. Injuries of the lower limbs caused by antipersonnel mines: the experience of the International Committee of the Red Cross. Injury. 1996;27(7):477–9.
Eardley WGP, Brown KV, Bonner TJ, Green AD, Clasper JC. Infection in conflict wounded. Philos Trans R Soc Lond B Biol Sci. 2011;366:204–18.
Hospenthal DR, Crouch HK, English JF, Leach F, Pool J, Conger NG, Whitman TJ, Wortmann GW, Robertson JL, Murray CK. Multidrug-resistant bacterial colonization of combat-injured personnel at admission to medical centers after evacuation from Afghanistan and Iraq. J Trauma. 2011;71(Suppl 1):S52–7.
Hospenthal DR, Murray CK, Andersen RC, Blice JP, Calhoun JH, Cancio LC, Chung KK, Conger NG, Crouch HK, D’Avignon LC, Dunne JR, Ficke JR, Hale RG, Hayes DK, Hirsch EF, Hsu JR, Jenkins DH, Keeling JJ, Martin RR, Moores LE, Petersen K, Saffle JR, Solomkin JS, Tasker SA, Valadka AB, Wiesen AR, Wortmann GW, Holcomb JB. Guidelines for the prevention of infection after combat-related injuries. J Trauma. 2008;64(3 Suppl):S211–20.
Couch KS, Stojadinovic A. Negative-pressure wound therapy in the military: lessons learned. Plast Reconstr Surg. 2011;127(Suppl 1):117S–30S.
Acknowledgments
The authors wish to acknowledge Farid H. for his participation in this study.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mathieu, L., Marty, A., Ramaki, A. et al. Current issues with lower extremity amputations in a country at war: experience from the National Military Hospital of Kabul. Eur J Trauma Emerg Surg 40, 387–393 (2014). https://doi.org/10.1007/s00068-013-0334-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-013-0334-y