
Abstract
Background and purpose
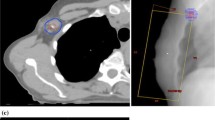
A bi-tangential technique is proposed to reduce undesired doses to the shoulder produced by standard tangential irradiation.
Patients and methods
A total of 6 patients affected by shoulder pain and reduced functional capacity after whole-breast irradiation were retrospectively analysed. The standard tangential plan used for treatment was compared with (1) a single bi-tangential plan where, to spare the shoulder, the lateral open tangent was split into two half-beams at isocentre, with the superior portion rotated by 10–20° medially with respect to the standard lateral beam; (2) a double bi-tangential plan, where both the tangential open beams were split. The planning target volume (PTV) coverage and the dose to the portion of muscles and axilla included in the standard tangential beams were compared.
Results
PTV95 % of standard plan (91.9 ± 3.8) was not significantly different from single bi-tangential plan (91.8 ± 3.4); a small but significant (p < 0.01) decrease was observed with the double bi-tangential plan (90.1 ± 3.7). A marked dose reduction to the muscle was produced by the single bi-tangential plan around 30–40 Gy. The application of the double bi-tangential technique further reduced the volume receiving around 20 Gy, but did not markedly affect the higher doses. The dose to the axilla was reduced both in the single and the double bi-tangential plans.
Conclusion
The single bi-tangential technique would have been able to reduce the dose to shoulder and axilla, without compromising target coverage. This simple technique is valuable for irradiation after axillary lymph node dissection or in patients without dissection due to negative or low-volume sentinel lymph node disease.
Zusammenfassung
Hintergrund und Ziel
Um die von tangentialer Standardbestrahlung produzierte unerwünschte Dosis in der Schulter zu reduzieren, wird vorgeschlagen, eine bitangentiale Technik zu verwenden.
Patienten und Methoden
Insgesamt 6 Patienten, die nach Bestrahlung der gesamten Brust an Schmerzen und reduzierter Funktionsfähigkeit der Schulter leiden, wurden retrospektiv analysiert. Der zur Bestrahlung verwendete tangentiale Standardbehandlungsplan wurde verglichen: (1) Mit einem einzel-bitangentialen Plan, wobei zur Schonung der Schulter, die laterale Tangente in zwei Felder im Isozentrum mittels „Half-Beam“-Technik aufgeteilt wurde. Der obere Abschnitt wurde dabei 10–20° medial in Bezug auf den lateralen Strahl gedreht. (2) Mit einem doppel-bitangentialen Plan, in dem beide tangentialen Felder aufgeteilt wurden. Die Planungszielvolumen-(PTV-)Abdeckung und die Dosis auf dem Abschnitt der Muskeln und der Achselhöhle, die in den tangentialen Standardfeldern erfasst waren, wurden verglichen.
Ergebnisse
PTV95 % der Standardpläne (91,9 ± 3,8) zeigten keine signifikanten Unterschiede im Vergleich zu einzel-bitangentialen Plänen (91,8 ± 3,4); eine kleine, aber signifikante (p < 0,01) Abnahme wurde mit dem doppel-bitangentialen Plan (90,1 ± 3,7) beobachtet. Eine deutliche Reduzierung der Dosis im Muskel wurde mit bitangentialen Plänen bei 30–40 Gy erreicht. Die Verwendung der doppel-bitangentialen Technik führte zu kleineren Volumen, welche 20 Gy erhielten, beeinflusste aber die Hochdosisbereiche nicht merklich. Die Dosis in der Achselhöhle wurde sowohl in den bitangentialen Plänen als auch in den doppel-bitangentialen Pläne reduziert.
Schlussfolgerung
Die bitangentiale Technik könnte die Dosis in der Schulter und Achselhöhle reduzieren, wobei die Dosis im Zielvolumen nicht beeinträchtigt wird. Diese einfache Technik ist geeignet für Bestrahlungen nach axillärer Lymphknotensektion oder aber auch für Patienten, für die keine Sektion vorgenommen wurde, da die Sentinellymphknoten nur gering oder gar nicht beeinträchtigt sind.



Similar content being viewed by others


References
Lundstedt D, Gustafsson M, Malmström P et al (2010) Symptoms 10–17 years after breast cancer radiotherapy data from the randomised SWEBCG91-RT trial. Radiother Oncol 97(2):281–287
Lauridsen MC, Overgaard M, Overgaard J et al (2008) Shoulder disability and late symptoms following surgery for early breast cancer. Acta Oncol 47(4):569–575
Hopwood P, Haviland JS, Sumo G et al (2010) Comparison of patient-reported breast, arm, and shoulder symptoms and body image after radiotherapy for early breast cancer: 5-year follow-up in the randomised Standardisation of Breast Radiotherapy (START) trials. Lancet Oncol 11(3):231–240
Ewertz M, Jensen AB (2011) Late effects of breast cancer treatment and potentials for rehabilitation. Acta Oncol 50(2):187–193
Yap KP, McCready DR, Narod S et al (2003) Factors influencing arm and axillary symptoms after treatment for node negative breast carcinoma. Cancer 97(6):1369–1375
Lee TS, Kilbreath SL, Refshauge KM et al (2008) Prognosis of the upper limb following surgery and radiation for breast cancer. Breast Cancer Res Treat 110(1):19–37
Blomqvist L, Stark B, Engler N, Malm M (2004) Evaluation of arm and shoulder mobility and strength after modified radical mastectomy and radiotherapy. Acta Oncol 43(3):280–283
Aristei C, Chionne F, Marsella AR et al (2001) Evaluation of level I and II axillary nodes included in the standard breast tangential fields and calculation of the administered dose: results of a prospective study. Int J Radiat Oncol Biol Phys 51(1):69–73
Alço G, Iğdem SI, Ercan T et al (2010) Coverage of axillary lymph nodes with high tangential fields in breast radiotherapy. Br J Radiol 83(996):1072–1076
Reznik J, Cicchetti MG, Degaspe B, Fitzgerald TJ (2005) Analysis of axillary coverage during tangential radiation therapy to the breast. Int J Radiat Oncol Biol Phys 61(1):163–168
Reed DR, Lindsley SK, Mann GN et al (2005) Axillary lymph node dose with tangential breast irradiation. Int J Radiat Oncol Biol Phys 61(2):358–364
Farace P, Zucca S, Solla I et al (2012) Planning hybrid intensity modulated radiation therapy for whole-breast irradiation. Int J Radiat Oncol Biol Phys 84(1):e115–e122
Norman SA, Localio AR, Potashnik SL et al (2009) Lymphedema in breast cancer survivors: incidence, degree, time course, treatment, and symptoms. J Clin Oncol 27(3):390–397
Deutsch M, Land S, Begovic M, Sharif S (2008) The incidence of arm edema in women with breast cancer randomized on the National Surgical Adjuvant Breast and Bowel Project study B-04 to radical mastectomy versus total mastectomy and radiotherapy versus total mastectomy alone. Int J Radiat Oncol Biol Phys 70(4):1020–1024
Nesvold IL, Fosså SD, Holm I et al (2010) Arm/shoulder problems in breast cancer survivors are associated with reduced health and poorer physical quality of life. Acta Oncol 49(3):347–353
Levangie PK, Drouin J (2009) Magnitude of late effects of breast cancer treatments on shoulder function: a systematic review. Breast Cancer Res Treat 116(1):1–15
Shamley D, Srinaganathan R, Oskrochi R et al (2009) Three-dimensional scapulothoracic motion following treatment for breast cancer. Breast Cancer Res Treat 118(2):315–322
Shamley DR, Srinanaganathan R, Weatherall R et al (2007) Changes in shoulder muscle size and activity following treatment for breast cancer. Breast Cancer Res Treat 106(1):19–27
Stubblefield MD (2011) Radiation fibrosis syndrome: neuromuscular and musculoskeletal complications in cancer survivors. PM R 3(11):1041–1054
Giuliano AE, Hunt KK, Ballman KV et al (2011) Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial. JAMA 305(6):569–575
Krag DN, Anderson SJ, Julian TB et al (2010) Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial. Lancet Oncol 11(10):927–933
Haffty BG, Hunt KK, Harris JR, Buchholz TA (2011) Positive sentinel nodes without axillary dissection: implications for the radiation oncologist. J Clin Oncol 29(34):4479–4481
Setton J, Cody H, Tan L et al (2012) Radiation field design and regional control in sentinel lymph node-positive breast cancer patients with omission of axillary dissection. Cancer 118(8):1994–2003
Compliance with ethical guidelines
Conflict of interest. P. Farace, M.A. Deidda, I. Iamundo, E. Deiana, R. Farigu, G. Lay and S. Porru state that there are no conflicts of interest.
The accompanying manuscript does not include studies on humans or animals.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Farace, P., Deidda, M., Iamundo de Curtis, I. et al. Bi-tangential hybrid IMRT for sparing the shoulder in whole breast irradiation. Strahlenther Onkol 189, 967–971 (2013). https://doi.org/10.1007/s00066-013-0428-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-013-0428-9