
Abstract
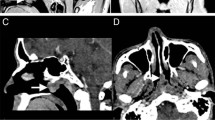
A 41-year-old male with primary hypothyroidism and a huge TSH-secreting pituitary tumor presented with a bleeding nasal mass that was initially misdiagnosed as a paraganglioma. Other unique features of the case include lack of complaints related to hypothyroidism, an extremely elevated TSH level of 3474 mU/l, and a low prolactin level. The presence of primary hypothyroidism made differentiating TSH-secreting pituitary adenoma from secondary thyrotroph hyperplasia difficult. A low molar ratio of α-subunit to TSH on presentation, together with normalization of TSH level and a 50% reduction in the size of the tumor after 6 weeks of thyroxine replacement therapy, suggested the presence of thyrotroph hyperplasia. However, the lack of further decrease in the size of the tumor that was associated with increased metabolic activity on 18-FDG PET scan, intense uptake on octreotide scan, and an elevated α-subunit to TSH molar ratio despite the normalization of free T4 and TSH levels for 16 months suggested the coexistence of thyrotroph adenoma. Together, the findings support the view that thyrotroph adenoma/ irreversible hyperplasia can result from long standing primary hypothyroidism.
Similar content being viewed by others


References
Khourides I.A., Weintraub B.D., Ridgway E.C., Maloof F. Pituitary secretion of free alpha and beta subunits of human thyrotropin in patients with thyroid disorders. J. Clin. Endocrinol. Metab. 1975, 40: 872.
Sarlis N.J., Brucker-Davis F., Doppman J.L., Skarulis M.C. MRI-demonstrable regression of a pituitary mass in a case of primary hypothyroidism after a week of acute thyroid hormone therapy. J. Clin. Endocrinol. Metab. 1997, 82: 808.
Katz M.S., Gregerman R.I., Horvath E., Kovacs E., Kovacs K., Ezrin C. Thyrotroph cell hyperplasia of the human pituitary gland associated with primary hypothyroidism: Clinical and morphological features. Acta Endocrinol. (Copenh.) 1980, 95: 41.
Langlois M.F., Lamarche J.B., Bellabarba D. Long-standing goiter and hypothyroidism: An unusual presentation of a TSH-secreting adenoma. Thyroid 1996, 6: 329.
Beck-Peccoz P., Brucker-Davis F., Persani L., Smallridge R.C., Weintraub B.D. Thyrotropin-secreting pituitary tumors. Endocr. Rev. 1996, 17: 610.
Kourides I.A., Ridgway E.C., Weintraub B.D., Bigos S.T., Gershengorn M.C., Maloof F. Thyrotropin-induced hyperthyroidism: Use of alpha and beta subunit levels to identify patients with pituitary tumors. J. Clin. Endocrinol. Metab. 1977, 45: 534.
Lamberts S.W.J., Krenning E.P., Reubi J.-C. The role of somatostatin and its analogs in the diagnosis and treatment of tumors. Endocr. Rev. 1991, 12: 450.
Halmi N.S., Gòude W.D. The morphogenesis of pituitary tumors induced by radiothyroidectomy in the mouse and effects of their transplantation on the pituitary body of the host. Am. J. Pathol. 1954, 30: 403.
Scheithaur B.W., Kovacs K., Randall R.V., Ryan N. Pituitary gland in hypothyroidism. Histologic and immunocytologic study. Arch. Pathol. Lab. Med. 1985, 109: 499.
Watanabe K., Kameya T., Yamauchi A., Yamamoto N., Kuwayama A., Takei I., Maruyama H., Saruta T. Thyrotropin-producing adenoma associated with pituitary resistance to thyroid hormone. J. Clin. Endocrinol. Metab. 1995, 76: 1025.
Zargar A.H., Masoodi S.R., Laway B.A., Shah N.A., Salahudin M. Familial puerperal alactogenesis: Possibility of a genetically transmitted isolated prolactin deficiency. Br. J. Obstet. Gynaecol. 1997, 104: 629.
D’Alessandro E., Santiemma V., Lore M.L., Ligas C., Del Porto G. 6p23 Deletion mosaicism in a woman with recurrent abortions and idiopathic hypoprolactinemia. Am. J. Med. Genet. 1992, 44: 220.
Zulewski H., Müller B., Exer P., Miserez A.R., Staub J.J. Estimation of tissue hypothyroidism by a new clinical score: Evaluation of patients with various grades of hypothyroidism and controls. J. Clin. Endocrinol. Metab. 1997, 82: 771.
Müller B., Zulewski H., Huber P., Ratcliffe J.G., Staub J.J. Impaired thyroid hormone action associated with smoking in women with hypothyroidism. N. Engl. J. Med. 1995, 333: 964.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Ghannam, N.N., Hammami, M.M., Muttair, Z. et al. Primary hypothyroidism-associated TSH-secreting pituitary adenoma/hyperplasia presenting as a bleeding nasal mass and extremely elevated TSH level. J Endocrinol Invest 22, 419–423 (1999). https://doi.org/10.1007/BF03343584
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03343584