
Abstract
Background and objective: Ideally, tests that predict the risk of cancer recurrence should be capable of guiding treatment decisions that are both therapeutically effective and cost effective. This paper evaluates the cost effectiveness of two tools that identify patients at high risk for biochemical (prostatespecific antigen) recurrence of prostate cancer after prostatectomy, the hypothesis being that accurate classification of high-risk patients will allow more appropriate use of secondary (adjuvant/salvage) treatment and may improve on current clinical practice. These risk-prediction tools are the Kattan postoperative nomogram, which uses clinicopathologic features, and the Prostate Px® test, which employs additional morphometric and immunofluorescence features of the prostate specimen to predict risk of biochemical recurrence. These tools were trained on patients treated at the Memorial Sloan-Kettering Cancer Center (996 patients for the nomogram, 342 patients for the Prostate Px® test).
Methods: The cost effectiveness of the Prostate Px® test, the Kattan postoperative nomogram, and current clinical practice were compared using a decision analytic model. The modeled treatment for low-risk patients was watchful waiting. The modeled treatments for high-risk patients were local radiation, hormonal therapy, and watchful waiting. Costs, utilities, and transition probabilities were obtained from the literature. Costs and effects were discounted at 3% per year. The time span modeled was 10 years after prostatectomy. Monte Carlo simulation was performed to estimate cost and effectiveness; sensitivity analysis was performed to examine the impact of uncertainty in the parameter values.
Results: The expected quality-adjusted life years (QALYs) for the Prostate Px® test, nomogram, and current practice were 8.11, 7.39, and 6.47, respectively. The expected costs were $US17 549, $US14 162, and $US14 104, respectively. The incremental cost-effectiveness ratio of the Prostate Px® was $US4704/QALY compared with the nomogram, and $US2100/QALY compared with current practice. The incremental cost-effectiveness ratio of the nomogram was $US63/QALY compared with current practice. These ratios are well below the common willingness-to-pay limit of $US50000/QALY. Expected effectiveness was highest for the Prostate Px® test, followed by the nomogram. Expected cost was slightly higher for Prostate Px® than for either alternative; nevertheless, the Prostate Px® was cost effective compared with both the nomogram and current practice. The nomogram was cost effective compared with current practice. The acceptable cost effectiveness of the Prostate Px® test and the nomogram compared with current practice were not sensitive to changes in the values used to inform the model within clinically plausible ranges. The superior performance of both Prostate Px® test and nomogram over current practice resulted from identifying high-risk patients likely to benefit from adjuvant treatment, while sparing the low-risk patients the added cost and toxicity of treatment.
Conclusion: Incorporation of risk-prediction tools in the initial management of patients after prostatectomy resulted in increased QALYs at an acceptable increase in cost relative to current practice.















Similar content being viewed by others

References
Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin 2008 Mar–Apr; 58(2): 71–96
Bolla M, van Poppel H, Collette L, et al. Postoperative radiotherapy after radical prostatectomy: a randomised controlled trial (EORTC trial 22911). Lancet 2005 Aug 13–19; 366(9485): 572–8
Messing EM, Manola J, Yao J, et al. Immediate versus deferred androgen deprivation treatment in patients with node-positive prostate cancer after radical prostatectomy and pelvic lymphadenectomy. Lancet Oncol 2006 Jun; 7(6): 472–9
Moul JW, Wu H, Sun L, et al. Early versus delayed hormonal therapy for prostate specific antigen only recurrence of prostate cancer after radical prostatectomy. J Urol 2004 Mar; 171(3): 1141–7
Thompson IM, Tangen CM, Paradelo J. Adjuvant radiotherapy for pathologically advanced prostate cancer: a randomized clinical trial. JAMA 2006; 296(19): 2329–35
Wiegel T, Bottke D, Willich N, et al. Phase III results of adjuvant radiotherapy (RT) versus “wait and see” (WS) in patients with pT3 prostate cancer following radical prostatectomy (RP) (ARO 96-02/AUO AP 09/95) [abstract no. 4513]. J Clin Oncol 2005 Jun; 23 (16S Pt I of II): 381
Stoch SA, Parker RA, Chen L, et al. Bone loss in men with prostate cancer treated with gonadotropin-releasing hormone agonists. J Clin Endocrinol Metab 2001 Jun; 86(6): 2787–91
Townsend MF, Sanders WH, Northway RO, et al. Bone fractures associated with luteinizing hormone-releasing hormone agonists used in the treatment of prostate carcinoma. Cancer 1997 Feb 1; 79(3): 545–50
Maillefert JF, Sibilia J, Michel F, et al. Bone mineral density in men treated with synthetic gonadotropin-releasing hormone agonists for prostatic carcinoma. J Urol 1999 Apr; 161(4): 1219–22
Oefelein MG, Ricchuiti V, Conrad W, et al. Skeletal fracture associated with androgen suppression induced osteoporosis: the clinical incidence and risk factors for patients with prostate cancer. J Urol 2001 Nov; 166(5): 1724–8
Hornberger J, Cosler LE, Lyman GH. Economic analysis of targeting chemotherapy using a 21-gene RT-PCR assay in lymph-node-negative, estrogenreceptor-positive, early-stage breast cancer. Am J Manag Care 2005 May; 11(5): 313–24
Shariat SF, Karakiewicz PI, Roehrborn CG, et al. An updated catalog of prostate cancer predictive tools. Cancer 2008 Dec 1; 113(11): 3075–99
Cordon-Cardo C, Kotsianti A, Verbel D, et al. Improved prediction of prostate cancer recurrence through systems pathology. J Clin Invest 2007; 117(7): 1876–83
Kattan MW, Wheeler TM, Scardino PT. Postoperative nomogram for disease recurrence after radical prostatectomy for prostate cancer. J Clin Oncol 1999 May; 17(5): 1499–507
Graefen M, Karakiewicz PI, Cagiannos I, et al. Validation study of the accuracy of a postoperative nomogram for recurrence after radical prostatectomy for localized prostate cancer. J Clin Oncol 2002 Feb 15; 20(4): 951–6
Stephenson AJ, Scardino PT, Eastham JA, et al. Postoperative nomogram predicting the 10-year probability of prostate cancer recurrence after radical prostatectomy. J Clin Oncol 2005 Oct 1; 23(28): 7005–12
Briggs A, Sculpher M. An introduction to Markov modelling for economic evaluation. Pharmacoeconomics 1998 Apr; 13(4): 397–409
Konski A, Watkins-Bruner D, Feigenberg S, et al. Using decision analysis to determine the cost-effectiveness of intensity-modulated radiation therapy in the treatment of intermediate risk prostate cancer. Int J Radiat Oncol Biol Phys 2006 Oct 1; 66(2): 408–15
Piper NY, Kusada L, Lance R, et al. Adenocarcinoma of the prostate: an expensive way to die. Prostate Cancer Prostatic Dis 2002; 5(2): 164–6
Krahn M, Ritvo P, Irvine J, et al. Patient and community preferences for outcomes in prostate cancer: implications for clinical policy. Med Care 2003 Jan; 41(1): 153–64
Shipley WU, Lu JD, Pilepich MV, et al. Effect of a short course of neoadjuvant hormonal therapy on the response to subsequent androgen suppression in prostate cancer patients with relapse after radiotherapy: a secondary analysis of the randomized protocol RTOG 86-10. Int J Radiat Oncol Biol Phys 2002 Dec 1; 54(5): 1302–10
Stephenson AJ, Shariat SF, Zelefsky MJ, et al. Salvage radiotherapy for recurrent prostate cancer after radical prostatectomy. JAMA 2004 Mar 17; 291(11): 1325–32
Catalona WJ, Smith DS. Cancer recurrence and survival rates after anatomic radical retropubic prostatectomy for prostate cancer: intermediate-term results. J Urol 1998 Dec; 160 (6 Pt 2): 2428–34
Berge V, Thompson T, Blackman D. Use of additional treatment for prostate cancer after radical prostatectomy, radiation therapy, androgen deprivation, or watchful waiting. Scand J Urol Nephrol 2007; 41(3): 198–203
Grossfeld GD, Li YP, Lubeck DP, et al. Predictors of secondary cancer treatment in patients receiving local therapy for prostate cancer: data from cancer of the prostate strategic urologic research endeavor. J Urol 2002 Aug; 168(2): 530–5
Fleming C, Wasson JH, Albertsen PC, et al. A decision analysis of alternative treatment strategies for clinically localized prostate cancer. Prostate Patient Outcomes Research Team. JAMA 1993 May 26; 269(20): 2650–8
Konski A, Watkins-Bruner D, Brereton H, et al. Long-term hormone therapy and radiation is cost-effective for patients with locally advanced prostate carcinoma. Cancer 2006 Jan 1; 106(1): 51–7
Konski A, Sherman E, Krahn M, et al. Economic analysis of a phase III clinical trial evaluating the addition of total androgen suppression to radiation versus radiation alone for locally advanced prostate cancer (Radiation Therapy Oncology Group protocol 86-10). Int J Radiat Oncol Biol Phys 2005 Nov 1; 63(3): 788–94
Scher HI, Kelly WM, Zhang ZF, et al. Post-therapy serum prostate-specific antigen level and survival in patients with androgen-independent prostate cancer. J Natl Cancer Inst 1999 Feb 3; 91(3): 244–51
Briggs A. Handling uncertainty in economic evaluation and presenting the results. In: Drummond M, Weinstein M, editors. Economic evaluation in health care: merging theory with practice. Oxford: Oxford University Press, 1991: 172–214
Doubilet P, Begg CB, Weinstein MC, et al. Probabilistic sensitivity analysis using Monte Carlo simulation: a practical approach. Med Decis Making 1985 Sum; 5(2): 157–77
Lipscomb J, Weinstein MC, Torrance GW. Time preference. In: Gold M, Siegel JE, Russell LB, et al., editors. Cost-effectiveness in health and medicine. Vol. 1. New York: Oxford University Press, 1996: 214–35
PDR Staff. 2006 Red Book: pharmacy’s fundamental reference (Red Book drug topics). Montvale (NJ): Thomson PDR, 2006
EuroQol. A new facility for the measurement of health-related quality of life: the EuroQol Group. Health Policy 1990; 16: 199–208
Tufts-New England Medical Center Institute for Clinical Research and Health Policy Studies. Preference weights 1998–2001 [online]. Available from URL: http://www.tufts-nemc.org/cearegistry/data/docs/phaseIIpreferenceweights.pdf [Accessed 2007 Mar 5]
Kuntz K, Weinstein M. Modelling in economic evaluation. In: Drummond M, McGuire A, editors. Economic evaluation in health care: merging theory with practice. Oxford: Oxford University Press, 2001: 141–71
Mehta SS, Lubeck DP, Sadetsky N, et al. Patterns of secondary cancer treatment for biochemical failure following radical prostatectomy: data from CaPSURE. J Urol 2004 Jan; 171(1): 215–9
Pass T, Goldstein L. A computerized aid for medical cost-effective analysis [abstract]. Med Decis Making 1981; 1: 465
Abramowitz MC, Pollack A. Postprostatectomy radiation therapy for prostate cancer. Semin Radiation Ocol 2008; 18(1): 15–22
Current Controlled Trials. Radiotherapy and androgen deprivation in combination after local surgery [ISRCTN40814031; online]. Available from URL: http://www.controlled-trials.com/ISRCTN40814031/40814031 [Accessed 2009 Feb 9]
Svateck RS, Lee JJ, Roehrborn CG, et al. The cost of prostate cancer chemoprevention: a decision analysis model. Cancer Epidemiol Biomarkers Prev 2006; 15(8): 1485–9
Calvert NW, Morgan AB, Catto JW, et al. Effectiveness and cost-effectiveness of prognostic markers in prostate cancer. Br J Cancer 2003; 88(1): 31–5
Moeremans K, Caekelbergh K, Annemans L. Cost-effectiveness analysis of bicalutamide (Casodex) for adjuvant treatment of early prostate cancer. Value Health 2004; 7(4): 472–81
Bayoumi AM, Brown AD, Garber AM. Cost-effectiveness of androgen suppression therapies in advanced prostate cancer. J Natl Cancer Inst 2000; 92(21): 1731–9
Ramsey S, Veenstra D, Clarke L, et al. Is combined androgen blockade with bicalutamide cost-effective compared with combined androgen blockade with flutamide? Urology 2005; 66(4): 835–9
Harrell Jr FE, Califf RM, Pryor DB, et al. Evaluating the yield of medical tests. JAMA 1982; 247(18): 2543–6
Acknowledgments
The study was supported by Aureon Laboratories, Inc. The authors confirm that the paper is an accurate representation of the study results. Aureon Laboratories, a privately held, venture capitalist-funded company headquartered in Yonkers, NY, USA, sells commercially the Prostate Px® test described in the paper. One of the authors, Valentina Bayer Zubek, is employed full-time as a Principal Machine Learning Scientist by Aureon Laboratories and has non-exercised stock options with Aureon Laboratories. The other author, Andre Konski, is the Chief Medical Officer of Fox Chase Cancer Center Partners, Philadelphia, PA, USA, and was employed as a consultant by Aureon Laboratories.
Aureon Laboratories directly funded the collection and management of the data. The study design, analysis and interpretation of the data, preparation, review, and approval of this manuscript were undertaken jointly by Drs Zubek and Konski. The publication of study results was not contingent on the sponsor’s approval. The data, models, and methodology developed for the Prostate Px® test and for this paper are proprietary to Aureon Laboratories. The authors thank Janet Novak of Helix Editing for her insightful comments while editing previous drafts of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Performance Metrics of the Risk-Prediction Tools
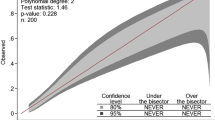
The concordance index[46] of the Prostate Px® test was 0.84 in the training cohort (342 patients) and 0.77 in the validation cohort (340 patients). The Prostate Px® test has sensitivity of 0.84 and specificity of 0.74 in the training cohort, and sensitivity of 0.77 and specificity of 0.72 in the validation cohort. The sensitivity and specificity are calculated relative to the threshold score that achieves the maximum product of sensitivity and specificity on the training set.
On the 342 patients used to train the Prostate Px® test, the nomogram’s concordance index was 0.73; on the 340 patients used to validate the Prostate Px® test, the nomogram’s concordance index was 0.79. On the entire training cohort of 996 patients, the nomogram’s concordance index was 0.88.[14] Note that the training and validation sets for the Prostate Px® test were used as validation sets on the Kattan nomogram when computing the metrics in Appendix table I, but they were part of the nomogram’s 996 training cohort. The nomogram’s authors did not report a threshold for calculating sensitivity and specificity. If a high-risk/low-risk cutpoint probability of 0.5 is considered, the nomogram’s sensitivity is 0.34 and specificity is 0.89 on the 342 training patients (with a sensitivity of 0.44 and specificity of 0.91 on the 340 validation patients); if the cutpoint that maximizes the product of sensitivity and specificity is considered, the nomogram’s sensitivity is 0.64 and the specificity is 0.74 on the 342 training patients (with a sensitivity of 0.64 and specificity of 0.83 on the 340 validation patients).
The performance metrics are summarized in Appendix table I. A summary of the prediction tools’ other characteristics is included in Appendix table II.
Though several accuracy measurements are provided in Appendix table I for the risk-prediction tools, the most appropriate one for survival analysis is the concordance index.[46] The concordance index is the generalization of the area under the receiver-operating characteristic (ROC) curve for survival data, and has an advantage over sensitivity and specificity by not depending on an arbitrary cutpoint that defines low/high risk.
Confidence Intervals around Cost, Effectiveness, and Incremental Cost-Effectiveness Ratios
Appendix table III presents the 95% confidence intervals around the cost and effectiveness of Prostate Px®, the nomogram, and current practice, and around their pairwise ICERs. Note that confidence intervals for costs are not paired, i.e. during simulation, one strategy might have a low cost and the other strategy might have a high cost, so comparing confidence intervals of costs is not informative. The same holds for comparing confidence intervals of effectiveness. For example, one strategy may always be less effective than another, for all data points in a simulation, yet their effectiveness ranges may overlap. Interpreting confidence intervals around ICER is especially tricky, even though they are below the $US50 000/QALY threshold. For example, the lower bounds of the confidence intervals around ICER_PX_CP and ICER_Nomo_CP (i.e. the ICER of Prostate Px® versus current practice, and the ICER of the nomogram versus current practice) in Appendix table III are negative because of the cheaper costs of the first strategy, which is also more effective and therefore the first strategy is dominant.
For cost-effectiveness analysis, both cost and effectiveness have to be considered. For all these reasons, it is better to analyze all data points from the Monte Carlo simulations by pairing two strategies; see, for example, the incremental cost-effectiveness scatterplots in figures 4–6.
Details of Sensitivity Analysis
Appendix tables IV and V present the ICERs of Prostate Px® versus the nomogram, Prostate Px® versus current practice, and the nomogram versus current practice, for low and high values of each variable in the model, taken within the clinically relevant range. Most of the time, the Prostate Px® and nomogram have ICERs lower than the willingness-to-pay threshold of $US50 000/QALY.
In the Monte Carlo simulation, each parameter is sampled from its distribution; the cost and effectiveness for Prostate Px®, the nomogram and current practice are calculated for each simulation. The base case for Monte Carlo simulation averages the cost and effectiveness over 1000 simulations, and then computes the ICERs. The roll-back base case estimates the cost and effectiveness by employing the mean value from each parameter’s distribution. In general, the Monte Carlo simulation average is the better ‘expected value’. However, we report the roll-back base case for comparison purposes because one-way sensitivity analysis changes the value of one parameter linearly within its range, and uses mean values for all the other parameters in its roll-back calculation. In other words, the ICER from sensitivity analysis should be compared with the base case from roll back, because sensitivity analysis uses roll back not Monte Carlo simulation in its estimates. When the ICER from sensitivity analysis is the same as the ICER in the base case from roll back, it means that the change in that parameter value did not affect the two compared strategies’ cost and effectiveness.
Clinical Effectiveness of Adjuvant Therapy after Prostatectomy
Three recent clinical prospective trials[2,5,6] demonstrated the benefit of adjuvant radiation therapy post-prostatectomy. The clinical trials randomized patients with high risk (positive margin and/or pT3) after radical prostatectomy to either radiation or observation. Adjuvant radiation significantly reduced the risk of biochemical recurrence in high-risk patients, compared with radical prostatectomy alone. Appendix table VI summarizes the studies’ findings.
Rights and permissions
About this article
Cite this article
Zubek, V.B., Konski, A. Cost Effectiveness of Risk-Prediction Tools in SelectingPatients for Immediate Post-Prostatectomy Treatment. Mol Diag Ther 13, 31–47 (2009). https://doi.org/10.1007/BF03256313
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03256313