
Abstract
Background
The survey of lifestyles, attitudes and nutrition (SLAN) is a national representative sample of 6,539 adults.
Aims
To report on both global and disease specific measures of self-reported morbidity according to age, gender and medical card status.
Methods
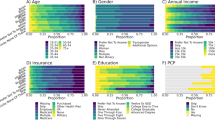
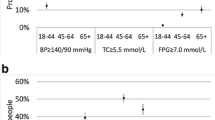
Reported rates of morbidity are given for angina, heart attack, stroke, raised blood pressure, cholesterol, diabetes mellitus and for other general conditions as well as difficulty with hearing and glasses/contact lens use. Stratified chi-squared analysis of categorical variables was conducted and logistic age adjusted regression model with general medical services (GMS) eligibility as the dependent variable.
Results
All conditions were more prevalent after the age of 45 years and showed a continuing age gradient. There were highly statistically significant inverse morbidity patterns according to GMS status among both men and women. Only reported raised cholesterol level was higher among the more affluent (13.5% males and 13.3% females over 45 years without a medical card, compared with 7.3% and 9.5% card holders respectively), one suggested explanation is the lack of access to means-tested screening.
Conclusions
There is considerable morbidity in the Irish population, particularly among GMS card holders.
Similar content being viewed by others

References
Building Healthier Hearts. The report of the cardiovascular strategy group.Department of Health and Children. Dublin. 1999.
Department of Health and Children. Dublin.Health Statistics. 1999. www.doh.h/statistics/health_statistics/health_status.html
Idler EL, Benyamini Y. Self-rated health and mortality: A review of twentyseven community studies.J Health Soc Behav 1997; 38: 21–37.
Heistaro S, Jousilahti P, Lahelma E, Vartiainen E, Pushka P. Self-rated health and mortality: a long-term prospective study in Eastern Finland.J Epidemiol Commun Health 2001; 55: 227–32.
Kuulasmaa K, Tunstall-Pedoe H, Dobson A et al. Estimation of contribution of changes in classic risk factors to trends in coronary event rates across the WHO MONICA Project populations.The Lancet 2000; 355: 675–87.
Friel S, Nic Gabhainn S, Kelleher CC. Main results of the national health and lifestyle surveys, SLAN and HBSC.Department of Health and Children Dublin and Centre for Health Promotion Studies Galway. 1999.
Shelley E, Daly L, Collins C et al. Cardiovascular risk factor changes in the Kilkenny Health Project, a community health promotion programme.European Heart J 1995; 16: 752–60.
Harrington KE, Robson PJ, Kiely M et al. The North/South Food Consumption Survey: Survey design and methodology.Public Health Nutrition 2001; 4 (5a): 1037–43.
Primatesta P, Brookes M, Poulter NR. Improved hypertension management and control — results from the Health Survey for England 1998.Hypertension 38(4): 827–32.
Creagh D, Neilson S, Collins A et al. Established cardiovascular disease and CVD risk factors in a primary care population of middle-aged Irish men and women. Submitted to theIrish Medical Journal.
Kelleher CC, Kingston SM, Cole M et al. Hypertension in diabetic clinic patients and their siblings.Diabetologia 1988; 31: 76–81.
Kelleher CC. Evolution of cardiovascular risk factors: light at the end of the tunnel?Wiener Klinische Wochenschrift: the Middle European Journal of Medicine 2001; 113: 549–54.
Colhoun HM, Dong W, Barakatt MT, Mather HM, Poulter NR. The scope for cardiovascular disease risk factor intervention among people with diabetes mellitus in England: a population-based analysis from the Health Surveys for England 1991–94.Diabetic Med 16(1): 35–40.
Lyons RA, O’Kelly J, Mason D et al. Social class and chronic disease in Dublin.Ir Med J 1996; 89: 174–6.
Howell F, O’Mahony M, Devlin J, O’Reilly O, Buttenshaw C. A geographical distribution of mortality and deprivation.Ir Med J 1993; 86: 96–9.
Johnson Z, Dack P. Small area mortality patterns.Ir Med J 1989; 82: 105–8.
Marmot M, Shipley M, Rose G. Inequalities in death; specific explanations or a general pattern:The Lancet 1984; 1: 1003–6.
Kennedy BP, Kawachi R, Glass R, Protherow-Stith D. Income distribution, socioeconomic status and self-rated health in the United States: multilevel analysis.Br Med J 1998; 317: 917–21.
Wilkinson RG. Unhealthy societies: the afflictions of inequality.Routledge. 1996.
Kelleher CC, Timoney A, Friel S, McKeown D. The relationship between indicators of deprivation, voting patterns and health status in the Republic of Ireland.J Epidemiol Commun Health 2002; 56: 36–44.
Tussing D. Irish medical care resources: an economic analysis. Dublin 1986.Economic and Social Research Institute paper number 126.
O’Shea E, Kelleher C. Health inequalities in Ireland. In: Rich and Poor. (Eds) Cantillon S et al. Combat Poverty Agency. Oak Tree Press. Dublin 2001.
Kelleher CC. Evaluating health promotion in three key settings. In: Quality, Evidence and Effectiveness in Health Promotion: grappling with uncertainties. (Eds)Davies JK and MacDonald M. Routledge. London 1999.
Hagan-Hennessy C, Moriarty DG, Zack MM, Scherr PA, Brackbill R. Measuring health-related quality of life for public health surveillance.Public Health Reports 1994; 109: 665–72.
Goldberg P, Gueguen A, Schamaus A, Nakache JP, Goldberg M. Longitudinal study of associations between perceived health status and selfreported diseases in the French Gazel cohort.J Epidemiol Commun Health 2001; 55: 233–8.
Chandola T, Jenkinson C. Validating self-rated health in different ethnic groups.Ethnicity Health 5(2): 151–9.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kelleher, C.C., Harrington, J. & Friel, S. Measures of self-reported morbidity according to age, gender and general medical services eligibility in the national survey of lifestyles, attitudes and nutrition. Ir J Med Sci 171, 134–138 (2002). https://doi.org/10.1007/BF03170499
Issue Date:
DOI: https://doi.org/10.1007/BF03170499