
Abstract
Purpose
To assess and compare the effects of normothermic and mild hypothermic cardiopulmonary bypass (CPB) on hepatosplanchnic oxygenation.
Methods
We studied 14 patients scheduled for elective coronary artery bypass graft surgery who underwent normothermic (> 35°C; group I,n = 7) or mild hypothermie (32°C; group II,n = 7) CPB. After induction of anesthesia, a hepatic venous catheter was inserted into the right hepatic vein to monitor hepatic venous oxygen saturation (ShvO2) and hepatosplanchnic blood flow by a constant infusion technique that uses indocyanine green.
Results
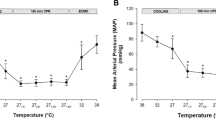
The ShvO2 decreased from a baseline value in both groups during CPB and was significantly lower at ten minutes and 60 min after the onset of CPB in group I (39.5 ± 16.2% and 40.1 ± 9.8%, respectively) than in group II (61.1 ± 16.2% and 6.0 ±17.9%, respectively;P < 0.05). During CPB, the hepatosplanchnic oxygen extraction ratio was significantly higher in group I than in group II (44.0 ± 7.2%vs 28.7 ±13.1%;P < 0.05).
Conclusion
Hepatosplanchnic oxygenation was better preserved during mild hypothermie CPB than during normothermic CPB.
Résumé
Objectif
Évaluer et comparer les effets de la circulation extracorporelle (CEC), sous normothermie ou hypothermie légère, sur l’oxygénation hépatosplanchnlque.
Méthode
Nous avons étudié 14 patients devant subir un pontage aortocoronarien avec CEC sous normothermie (> 35 °C; groupe I, n = 7) ou hypothermie légère (32 °C; groupe II, n = 7). Après l’induction de l’anesthésle, un cathéter a été inséré dans la veine hépatique droite pour permettre de vérifier la saturation en oxygène du sang veineux hépatique (SO2vh) et le débit sanguin hépatosplanchnlque par une perfusion constante utilisant le vert d’indocyanlne.
Résultats
La SO2vh a diminué de sa valeur de base dans les deux groupes et a été significativement plus basse à 10 minutes et à 60 min après le début de la CEC dans le groupe I (39,5 ± 16,2 % et 40,1 ± 9,8 %, respectivement) que dans le groupe II (61,1 ± 16,2 % et 61,0 ± 17,9 %, respectivement; P < 0,05). Le taux déxtraction d’oxygène hépatosplanchnlque pendant la CEC a été significativement plus élevé dans le groupe I que dans le groupe II (44,0 ± 7,2 % vs 28,7 ± 13,1 %; P < 0,05).
Conclusion
Loxygénation hépatosplanchnlque a été mieux préservée pendant la CEC sous hypothermie légère que sous normothermie.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Cook DJ. Changing temperature management for cardiopulmonary bypass. Anesth Analg 1999; 88: 1254–71.
Thorén A, Elam M, Ricksten S-E. Jejunal mucosal perfusion is well maintained during mild hypothermic cardiopulmonary bypass in humans. Anesth Analg 2001; 92: 5–11.
McNicol L, Andersen LW, Liu G, Doolan L, Baek L. Markers of splanchnic perfusion and intestinal translocation of endotoxins during cardiopulmonary bypass: effects of dopamine and milrinone. J Cardiothorac Vasc Anesth 1999; 13: 292–8.
Okano N, Fujita N, Kadoi Y, Saito S, Goto F. Disturbances in hepatocellular function during cardiopulmonary bypass using propofol anesthesia. Eur J Anaesth 2001; 18: 1–7.
Bradley SE, Ingelfinger FJ, Bradley GP, Curry JJ. The estimation of hepatic blood flow in man. J Clin Invest 1945; 24: 890–7.
Landow L, Phillips DA, Heard SO, Prevost D, Vandersalm TJ, Fink MP. Gastric tonometry and venous oximetry in cardiac surgery patients. Crit Care Med 1991; 19: 1226–33.
Haisjackl M, Birnbaum J, Redlin M, et al. Splanchnic oxygen transport and lactate metabolism during normothermic cardiopulmonary bypass in humans. Anesth Analg 1998; 86: 22–7.
Takala J. Determinants of splanchnic blood flow. Br J Anaesth 1996;77: 50–8.
Pastor CM, Suter PM. Hepatic hemodynamics and cell functions in human and experimental sepsis. Anesth Analg 1999; 89: 344–52.
Kainuma M, Fujiwara Y, Kimura N, Shitaokoshi A, Nakashima K, Shimada Y. Monitoring hepatic venous hemoglobin oxygen saturation in patients undergoing liver surgery. Anesthesiology 1991; 74: 49–52.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Okano, N., Hiraoka, H., Owada, R. et al. Hepatosplanchnic oxygenation is better preserved during mild hypothermic than during normothermic cardiopulmonary bypass. Can J Anaesth 48, 1011–1014 (2001). https://doi.org/10.1007/BF03016592
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03016592