
Abstract
Purpose
To compare two doses of bolus epidural morphine with bolus iv morphine for postoperative pain after abdominal or genitourinary surgery in infants.
Methods
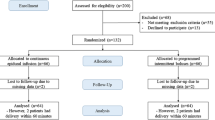
Eighteen infants were randomly assigned to bolus epidural morphine (0.025 mg · kg−1 or 0.050 mg · kg−1) or bolus iv morphine (0.050–0.150 mg · kg−1). Postoperative pain was assessed and analgesia provided, using a modified infant pain scale. Monitoring included continuous ECG, pulse oximetry, impedance and nasal thermistor pneumography. The CO2 response curves and serum morphine concentrations were measured postoperatively.
Results
Postoperative analgesia was provided within five minutes by all treatment methods. Epidural groups required fewer morphine doses (3.8 ± 0.8 for low dose [LE], 3.5 ± 0.8 for high dose epidural [HE] vs. 6.7 ± 1.6 for iv, P < 0.05) and less total morphine (0.11 ± 0.04 mg · kg−1 for LE, 0.16 ± 0.04 for HE vs 0.67 ± 0.34 for iv, P < 0.05) on POD1 Dose changes were necessary in all groups for satisfactory pain scores. Pruritus, apnoea, and haemoglobin desaturation occurred in all groups. CO2 response curve slopes, similar preoperatively (range 36–41 ml · min−1 · mmHg ETco −12 · kg−1) were generally depressed (range, 16–27 ml · min−1 · mmHg ETco −12 · kg−1) on POD1. Serum morphine concentrations, negligible in LE (<2 ng · ml−1), were similar in the HE and iv groups (peak 8.5 ± 12.5 and 8.6 ± 2.4 ng · ml−1, respectively).
Conclusion
Epidural and iv morphine provide infants effective postoperative analgesia, although side effects are common. Epidural morphine gives satisfactory analgesia with fewer doses (less total morphine); epidural morphine 0.025 mg · kg−1 is appropriate initially. Infants receiving epidural or iv morphine analgesia postoperatively need close observation in hospital with continuous pulse oximetry.
Résumé
Objectif
Comparer deux doses épidurales de morphine en bolus avec un bolus de morphine iv administrées pour la douleur postopératoire après une chirurgie abdominale ou urogénitale chez l’enfant.
Méthodes
Dix-huit enfants ont été répartis pour recevoir soit un bolus de morphine épidural (0,025 mg · kg−1 ou 0,05 mg · kg−1) soit un bolus de morphine iv (0,050–0,150 mg · kg−1). La douleur postopératoire était évaluée et l’analgésie pourvue sur la basé d’une échelle de douleur modifée pour la pédiatrie. Le monitorage incluait l’ECG continu, l’oxymétrie de pouls, la pneumographie par impédance avec un thermistor nasal. En postopératoire, on mesurait les courbes de réponse au CO2 et les concentrations sériques de morphine.
Résultats
L’analgésie postopératoire survenait en déçà de cinq minutes, indépendamment du traitement administré. Un nombre inférieur de doses de morphine (3,8 ± 0,8 pour la dose légère [DL], 3,5 ± 0,8 pour la dose forte [DF] vs 6,7 ± 1,6 pour la morphine iv, P < 0,05) à demande a été requis pour les groupes recevant la morphine épidurale. Pour obtenir des scores satisfaisants sur l’échelle de la douleur, on a dû modifier les doses dans tous les groupes. On a noté du prurit, de l’apnée et une désaturation en oxygène dans tous les groupes. Les courbes identiques en préopératoire de la réponse au CO2 (écart, 36–41 ml · min−1 · mmHg ETco −12 · kg−1) étaient généralement déprimées (écart, 16–27 ml · min−1 · mmHg ETco −12 · kg−1). Les concentrations de morphine sérique, négligeables pour DL (<2 ng · ml−1), étaient identiques pour DF et iv (maximum respectif 8,5 ± 12,5 et 8,6 ± 1,4 ng · ml−1).
Conclusion
La morphine épidurale et la morphine iv procurent une analgésie postopératoire suffisante aux enfant malgré des effets secondaires fréquents. La morphine épidurale a produit une analgésie satisfaisante nécessitant moins de doses (dose totale moindre); la morphine épidurale 0,025 mg · kg−1 est appropriée au début. Les enfants qui reçoivent de la morphine épidurale ou iv comme analgésique postopératoire doivent être surveillés de près à l’hôpital avec l’oxymétrie de pouls en continu.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Attia J, Ecoffey C, Sandouk P, Gross JB, Samii K. Epidural morphine in children: pharmacokinectics and CO2 sensitivity. Anesthesiology 1986; 65: 590–4.
Haberkern CM, Tyler DC, Krane EJ. Postoperative pain management in children. Mt Sinai J Med 1991; 58: 247–56.
Clenski JA, Warner MA, Dawson B, Kaufman B. Postoperative use of epidurally administered morphine in children and adolescents. Mayo Clin Proc 1984; 59: 530–3.
Krane EJ, Jacobson LE, Lynn AM, Parrot C, Tyler DC. Caudal morphine for postoperative analgesia in children: a comparison with caudal bupivacaine and intravenous morphine. Anesth Analg 1987; 66: 647–53.
Krane EJ, Tyler DC, Jacobson LE. The dose response of caudal morphine in children. Anesthesiology 1989; 71: 48–52.
Rasch DK, Webster DE, Pollard TG, Gurkowski MA. Lumbar and thoracic epidural analgesia via the caudal approach for postoperative pain relief in infants and children. Can J Anaesth 1990; 37: 359–62.
Rosen KR, Rosen DA. Caudal epidural morphine for control of pain following open heart surgery in children. Anesthesiology 1989; 70: 418–21.
Valley RD, Bailey AG. Caudal morphine for postoperative analgesia in infants and children: a report of 138 cases. Anesth Analg 1991; 72: 120–4.
Bhat R, Chah G, Gulati A, Aldana O, Velamati R, Bhargava H. Pharmacokinetics of a single dose of morphine in preterm infants during the first week of life. J Pediatr 1990; 117: 477–81.
Lynn AM, Slattery JT. Morphine pharmacokinetics in early infancy. Anesthesiology 1987; 66: 136–9.
Meistelman C, Benhamou D, Barre J, et al. Effects of age on plasma protein binding of sufentanil. Anesthesiology 1990; 72: 470–3.
Way WL, Costley EC, Way EL. Respiratory sensitivity of the newborn infant to meperidine and morphine. Clin Pharmacol Ther 1964; 6: 454–61.
Barrier G, Attia J, Mayer MN, Amiel-Tison C, Shnider SM. Measurement of post-operative pain and narcotic administration in infants using a new clinical scoring system. Intensive Care Med 1989; 15: S37–9.
Grunau RVE, Craig KD. Facial activity as a measure of neonatal pain expression. Advances in Pain Research Therapy 1990; 15: 147–55.
Lynn AM, Nespeca MK, Opheim KE, Slattery JT. Respiratory effects of intravenous morphine infusions in neonates, infants, and children after cardiac surgery. Anesth Analg 1993; 77: 695–701.
Lynn AM, Opheim KE, Tyler DC. Morphine infusion after pediatric cardiac surgery. Crit Care Med 1984; 12: 863–7.
Gibaldi M, Perrier D. Pharmacokinetics, 2nd ed. New York: Marcel Dekker, 1982: 319–53.
Dalens B, Tanguy A, Haberer J-P. Lumbar epidural anesthesia for operative and postoperative pain relief in infants and young children. Anesth Analg 1986; 65: 1069–73.
Serlin S. Single-dose caudal epidural morphine in children: safe, effective, and easy. J Clin Anesth 1991; 3: 386–90.
Hoppenbrouwers T, Hodgman JE, Harper RM, Hoffman E, Sterman MB, McGinty DJ. Polygraphic studies of normal infants during the first six months of life: III. Incidence of apnea and periodic breathing. Pediatrics 1977; 60: 418–25.
Tyler DC, Woodham M, Stocks J, Leary A, Lloyd-Thomas A. Oxygen saturation in children in the postoperative period. Anesth Analg 1995; 80: 14–9.
Hug CC Jr. Pharmacokinetics and dynamics of narcotic analgesics. In: Prys-Roberts C, Hug CC Jr (Eds.). Pharmacokinetics of Anaesthesia. Oxford: Blackwell Scientific Publications, 1984: 187–234.
Avery ME, Chernick V, Dutton RE, Permutt S. Ventilatory response to inspired carbon dioxide in infants and adults. J Appl Physiol 1963; 18: 895–903.
Olsen GD, Lees MH. Ventilatory response to carbon dioxide of infants following chronic prenatal methadone exposure. J Pediatr 1980; 96: 983–9.
Nichols DC, Yaster M, Lynn AM, et al. Disposition and respiratory effects of intrathecal morphine in children. Anesthesiology 1993; 79: 733–8.
McRorie TI, Lynn AM, Nespeca MK, Opheim KE, Slattery JT. The maturation of morphine clearance and metabolism. American Journal of Diseases of Children 1992; 146: 972–6.
Pokela M-L, Olkkola KT, Seppälä T, Koivisto M. Agerelated morphine kinetics in infants. Dev Pharmacol Ther 1993; 20: 26–34.
Zakowski MI, Ramanathan S, Turndorf H. A two-dose epidural morphine regimen in cesarean section patients: pharmacokinetic profile. Acta Anaesthesiol Scand 1993; 37: 584–9.
Coté CJ, Zaslavsky A, Downes JJ, et al. Postoperative apnea in former preterm infants after inguinal herniorrhaphy. Anesthesiology 1995; 82: 809–22.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by BRSG Grant #RR05655-20.
Rights and permissions
About this article
Cite this article
Haberkern, C.M., Lynn, A.M., Geiduschek, J.M. et al. Epidural and intravenous bolus morphine for postoperative analgesia in infants. Can J Anaesth 43, 1203–1210 (1996). https://doi.org/10.1007/BF03013425
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03013425