
Abstract
Purpose
The onset of anterior cervical myelopathy in the early postoperative period is an unusual complication after cardiac surgery without extracorporeal circulation in which haemodynamic stability was maintained. We report a patient who developed anterior cervical myelopathy after cardiac surgery.
Clinical features
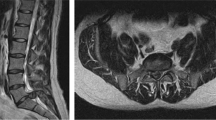
A 53-yr-old man with no serious associated medical problems underwent cardiac surgery without extracorporeal circulation to repair a ruptured left ventricle. Haemodynamic stability was maintained throughout the procedure but the patient developed flaccid paraparesis and dissociated sensory loss, three hours later Early recognition of the clinical picture and prompt initiation of steroid treatment facilitated a successful outcome. The definitive diagnosis was based on magnetic resonance findings days after surgery.
Conclusion
The onset or aggravation of neurological symptoms in the postoperative period may be avoided by thorough search for medullary pathology in the patient’s background and by using particular care when performing manoeuvres dunng the penoperative period, not only to ensure haemodynamic stability, thus preserving medullary perfusion, but also to avoid mechanical compression of a spinal segment.
Résumé
Objectif
L’apparition à la période postopératoire d’une myélopathie cervicale antérieure constitue une complication inusitée pour une intervention cardiaque sans circulation extracorporelle (CEC) et sans altération de la stabilité hémodynamique. Nous rapportons le cas d’un patient victime d’une myélopathie cervicale après une ch churgie cardiaque.
Éléments cliniques
Un homme de 53 sans problèmes médicaux associés importants a subi une chirurgie sans CEC pour la réparation d’une rupture ventriculaire gauche. La stabilité hémodynamique a été maintenue pendant l’intervention mais le patient a développé une paraparésie flasque et une perte de sensibilité dissociée trois heures après l’intervention. La reconnaissance précoce du tableau clinique et l’initiation rapide de la corticothérapie a permis une évolution favorable.
Conclusion
À la période postopératoire, l’apparition et l’aggravation de symptômes neurologiques peuvent être évitées par la recherche méticuleuse d’une pathologie médullaire préalable. Pendant la période périopératoire. il faut assurer la stabilité hémodynamique et éviter la compression mécanique du rachis.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Skouen JS, Wainapel SF, Willock MM. Paraplegia following epidural anesthesia. A case report and a literature review. Acta Neurol Scand 1985; 72: 437–43.
Singh U, Silver JR, Welply NC. Hypotensive infarction of the spinal cord. Paraplegia 1994; 32: 314–22.
Mills GH, Howell SJL, Richmond MN. Spinal cord compression inmediately following, but unrelated to, epidural analgesia. Anaesthesia 1994; 49: 954–6.
Woodall N, Huggins NJ, Jewkes DA. Postoperative paraplegia in a patient with an unsuspected dural arterio-venous malformation. Br J Anaesth 1990; 64: 638–41.
Arbonés Arán E, Espinosa Soldevilla W, Gutiérrez de Simone JW, Molina Ros A, Ardevol Cuesta J. Anterior spinal artery syndrome and intradural anesthesia. (Spanish) Rev Esp Anestesiol Reanim 1987; 34: 221–4.
Foster MR, Nimmo GR, Brown AG. Prolapsed intervertebral disc after epidural analgesia in labour. Anaesthesia 1996; 51: 773–5.
Stutesman JL, Houston JM, Wayne DA. Post-surgical ischaemic myelopathy. Paraplegia 1987; 25: 23–6.
Silver JR, Buxton PH. Spinal stroke. Brain 1974; 97: 539–50.
Albin MS. Spinal cord injury.In: Cottrell JE, Smith DS (Eds.). Anesthesia and Neurosurgery, 3rd ed. St. Louis: Mosby 1993: 713–43.
Sawin PD, Todd MM, Traynelis VC, et al. Cervical spine motion with direct laryngoscopy and orotracheal intubation. Anesthesioloy 1996; 85: 26–36.
Miller RA, Crosby G, Sundaram P. Exacerbated spinal neurologic deficit during sedation of a patient with cervical spondylosis. Anesthesiology 1987; 67: 844–6.
Laraki M, Orliaguet GA, Flandin C, Merckx J, Barrier G. Hysterical paraplegia as a cause of transient paraplegia after epidural anesthesia. Anesth Analg 1996; 83: 876–7.
Fisiopatología de la médula y de las raices nerviosas. En Ráibano Navas AD. Guión de fisiopatología del sistema nervioso. Artes Gráficas Benzal, SA. Univ. Alcalá de Henares. Madrid. 1980: 6–35.
Errea JM, Ara JR, Pina MA, Fayed N. Anterior spinal artery syndrome due to cervical disk protrusion. Diagnosis by magnetic resonance. (Spanish). Neurología 1991; 6: 256–8.
Netter FH. Sistema nervioso. Anatomía y fisiología. Vascularizaciôn de la médula espinal. Colección CIVA de llustraciones Médica, 2nd ed. Ed Salvat, Barcelona, 1986. Tomo I-1: 64–6.
Gillilan LA. Veins of the spinal cord. Anatomic details; suggested clinical applications. Neurology 1970; 20: 860–7.
Taneichi H, Abumi K, Kaneda K, Terae S. Monitoring the evolution of intramedullary lesions in cervical spinal cord injury. Qualitative and quantitative analysis with sequential MR imaging. Paraplegia 1994; 32: 9–18.
Troianos CA, Kuwik RJ, Pasqual JR, Lim AJ, Odasso DP. Internal jugular vein and carotid artery anatomic relation as determined by ultrasonography. Anesthesiology 1996; 85: 43–8.
Chiles BW III, Cooper PR. Acute spinal injury. N Engl J Med 1996; 334: 514–20.
Hickey R, Sloan TB, Albin MS. Acute spinal cord trauma.In: Shoemaker WC (Ed.). Textbook of Critical Care, 3rd ed. Philadelphia, Pennsylvania: WB Saunders Company, 1995; 158: 1457–65.
Seingry DR. Cervical injuries-anaesthetic implications, monitoring and management. Baillière’s Clinical Anaesthesiology 1987; 1: 459–76.
Fujinma Y, Nishi T, Chiba K, Kobayashi K. Prognosis of neurological deficits associated with upper cervical spine injuries. Paraplegia 1995; 33: 195–202.
Toscano J. Prevention of neurological deterioration before admission to a spinal cord injury unit. Paraplegia 1988; 26: 143–50.
Kelly DF. Steroids in head injury. New Horiz 1995; 3: 453–5.
Waring WP, Karunas RS. Acute spinal cord injuries and the incidence of clinically ocurring thromboembolic disease. Paraplegia 1991; 29: 8–16.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Muñoz, C.L., del García, V.S., Gonzalez, A. et al. Anterior cervical myelopathy in the early postoperative period. Can J Anaesth 44, 872–876 (1997). https://doi.org/10.1007/BF03013164
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03013164