
Abstract
Objective:To determine the rate and predictors of clinician compliance with treatment guidelines for high cholesterol in a primary care practice and establish quality assurance thresholds for monitoring patient management.
Design:Retrospective chart audit one year after high (>240 mg/dL) cholesterol level.
Patients:257 (243 after exclusions) consecutive patients with serum cholesterol levels greater than 240 mg/dL.
Setting:Primary care practice of group-model university-based HMO.
Interventions:None.
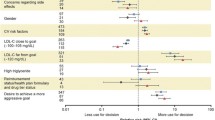
Measurements and main results:In the one-year interval following the index elevated cholesterol level, 67% of 243 patients had received documented dietary counseling, 53% had had a follow-up cholesterol test, and 8% were started on drug treatment. Only two patients (1.8%) without a history of hypercholesterolemia prior to the index level were started on drug treatment, compared with 18 patients (15%) with such a history. The odds (and 95% confidence intervals) of patient dietary counseling increased twofold (1.35 to 2.95) for each 25-mg/dL increment in serum cholesterol, and by 1.45 times (1.12 to 1.87) for each additional coronary risk factor. Patients who had high cholesterol levels obtained as isolated determinations bad 2.46 times (1.32 to 4.64) higher odds of being followed by counseling than did those whose levels had been obtained as part of a chemistry panel.
Conclusions:Compliance with National Cholesterol Education Panel guidelines for dietary counseling, but not drug therapy, was higher in this setting than in other published compliance studies. Quality assurance monitoring of compliance with dietary counseling and obtaining lipid measurements using a threshold approach are suggested. A similar approach to drug therapy of hypercholesterolemia appears premature.
Similar content being viewed by others


References
National Institutes of Health Consensus Conference on Cholesterol Lowering. Lowering blood cholesterol to prevent heart disease. JAMA 1985;253:2080–6.
Superko HR, Desmond DA, de Santos VV, et al. Blood cholesterol treatment attitudes of community physicians: a major problem. Am Heart J. 1988;116(3):849–55.
Schucker B, Wittes JT, Cutler JA, et al. Change in physician perspective on cholesterol and heart disease: results from two national surveys. JAMA. 1987;258:3521–6.
Yates K, Jackson R, Tester P, et al. Serum cholesterol and coronary heart disease: Auckland general practitioners’ attitudes and practices in 1986. N Z Med J. 1988;101:76–8.
Vivier PM, Dietrich AJ, Witters LA. Management of elevated cholesterol levels by New Hampshire primary care physicians. J Fam Pract. 1988;27(2):167–72.
Madlon-Kay DJ. Family physician recognition and treatment of severe hypercholesterolemia. J Fam Pract 1987;24(1):54–6.
Whiteside C, Robbins JA. Cholesterol knowledge and practices among patients compared with physician management in a university primary care setting. Prev Med. 1989;18:526–31.
Nichols AW. Management of elevated serum cholesterol in a university-based family practice. J Fam Pract. 1988;26(3):281–5.
Bell MM, Dippe SE. Recognition and treatment of hypercholesterolemia in a family practice center. J Fam Pract. 1988;26(5):507–13.
Madlon-Kay DJ. Improvement in family physician recognition and treatment of hypercholesterolemia. Arch Intern Med. 1989;149:1754–5.
National Cholesterol Education Program Expert Panel. Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Arch Intern Med. 1988;148:36–55.
Marder RJ. Commentary: relatinoship of clinical indicators and practice guidelines. QRB 1990;16(2):60.
Joint Commission on Accreditation of Healthcare Organizations. Characteristics of clinical indicators. QRB 1989;15(11):330–9.
Miaskowski C. Quality assurance issues in oncology nursing. Cancer. 1989;64:285–9.
Fauman MA. Quality assurance monitoring in psychiatry. Am J Psychiatry. 1989;146(9):1121–30.
Larsen RD, Bennion SD, Leonard TE. Monitoring and evaluation in an army health clinic. QRB. 1989;15:238–45.
Himmelstein DU, Woolhandler S. Free care, cholestyramine, and health policy. N Engl J Med. 1984;311:1511–4.
Becker MH. The cholesterol saga: whither health promotion? Ann Intern Med. 1987;106(4):623–6.
Zwelg S. An opposing view. J Fam Pract. 1988;26(6):670–5.
Thompson PD. Putting cholesterol control on a diet. JAMA. 1989;262:2998.
Corday E, Ryden L. Why some physicians have concerns about the Cholesterol Awareness Program. J Am Coll Cardiol. 1989;13(2):497–502.
Lomas J, Anderson GM, Domnick-Pierre K, Vayda E, Enkin MW, Hannah WJ. Do practice guidelines guide practice? The effect of a consensus statement on the practice of physicians. N Engl J Med. 1989;321:1306–11.
Goldman L. Changing physicians’ behavior: the pot and the kettle [editorial]. N Engl J Med. 1990;322:1524–5.
Author information
Authors and Affiliations
Additional information
Received from the Department of Health Care Sciences, George Washington University Medical Center, Washington, DC.
Rights and permissions
About this article
Cite this article
Schectman, J.M., Elinsky, E.G. & Bartman, B.A. Primary care clinician compliance with cholesterol treatment guidelines. J Gen Intern Med 6, 121–125 (1991). https://doi.org/10.1007/BF02598306
Issue Date:
DOI: https://doi.org/10.1007/BF02598306