
Abstract
The prevalence of chlamydial infection and associated risk factors were studied in 1531 women from ten clinics in New York State excluding New York City. OverallChlamydia infection rates were 13.6%; 17.6% in eight high risk family planning and STD clinics, and 5.7% in two low risk college and private clinics. Risk factors forChlamydia infection included: age <20 years (odds ratio 1.6), use of oral contraceptives (odds ratio 2.0), a history of having more than one sexual partner (odds ratio 1.7) and, in one clinic where data was available, inflammation on Papanicolaou smears (odds ratio 2.1).
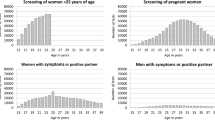
These data helped secure funding forChlamydia preventive services and permitted development of a risk profile (score card) ofChlamydia for each age group. Use of such a score card can be most helpful in assigning which patients could benefit most fromChlamydia cultures, especially in those areas where testing is unavailable or too costly to screen all patients.
Similar content being viewed by others


References
McCormack WM, Alpert S, McComb DE, Nichols RL, Semine DZ, Zinner SH. Fifteen month study of women infected withChlamydia trachomatis. N Eng J Med300: 123–5, 1979.
Washington AE, Johnson RE, Sanders LL.Chlamydia trachomatis infections in the United States. What are they costing us? JAMA257: 2070–2, 1986.
Richmond SJ, Paul ID, Taylor PK. Value and feasibility of screening women attending STD clinics for cervical chlamydial infections. Br J Vener Dis56: 92–5, 1980.
Handsfield HH, Jasman LL, Roberts PL, Hanson VW, Kothenbeutel RL, Stamm WE. Criteria for selective screening forChlamydia trachomatis infection in women attending family planning clinics. JAMA255: 1730–4, 1986.
Harrison RH, Costin M, Meder JB et al. CervicalChlamydia trachomatis infection in university women: Relationship to history, contraception, ectopy, and cervicitis. Am J Obstet Gynecol153: 244–51, 1985.
Arya OP, Mallinson H, and Goddard AD: Epidemiological and clinical correlates of chlamydial infection of the cervix. Br J Vener Dis57: 118–24, 1981.
Chacko MR, Lovchik JC:Chlamydia trachomatis infection in sexually active adolescents: prevalence and risk factors. Pediatrics73: 836–40, 1984.
Shafer MA, Beck A, Blain B, et al.Chlamydia trachomatis: Important relationships to race, contraception, lower genital tract infection, and Papanicolaou smear. J Pediatr104: 141–6, 1984.
Washington AE, Gove S, Schachter J, Sweet RL. Oral Contraceptives,Chlamydia trachomatis infection, and pelvic inflammatory disease. JAMA253: 2246–50, 1985.
Kinghorn GR and Waugh MA. Oral contraceptive use and prevalence of infection withChlamydia trachomatis in women. Br J Vener Dis57: 187–90, 1981.
Hipp SS, Han Y, Murphy D. Assessment of Enzyme Immunoassay and Immunofluorescence Tests for Detection ofChlamydia trachomatis. J Clin Microbiol25: 1938–43, 1987.
Chernesky MA, Mahony JB, Castriciano S, Mores M, Stewart IO, Landis SJ, Seidelman W, Sargeant EJ, Leman C. Detection ofChlamydia trachomatis antigens by enzyme immunoassay and immunofluorescence in genital specimens from symptomatic and asymptomatic men and women. J Infect Dis154: 141–8, 1986.
Edwards D, Phillips D, Stancomb S:Chlamydia trachomatis infection at a family planning clinic. N Z Med J98: 333–5, 1985.
Berg AD, Heidrich EF, Fihn SD et al. Establishing the cause of genitourinary symptoms in women in a family practice; comparison of clinical examination and comprehensive microbiology. JAMA25: 620–5, 1984.
Tam MR, Stamm WE, Handsfield HH et al. Culture-independent diagnosis ofChlamydia trachomatis using monoclonal antibodies. N Eng J Med310: 1146–50, 1984.
Jones MF, Smith TF, Houglum AJ, Herrmann JE.Detection of Chlamydia trachomatis in genital specimens by the Chlamydiazyme test. J Clin Microbiol20: 465–711, 1984.
Hipp SS. Laboratory technique for identification ofChlamydia trachomatis. In Sexually Related Infectious Disease. Sun T (Ed.) Yearbook Med Pub, New York 161–71, 1986.
Sompolinsky D, Richmond S. Growth ofChlamydia trachomatis in McCoy cells treated with cytochalasin B. Appl Microbiol28: 912–4, 1974.
Ripa KV, Mårdh P-A. Cultivation ofChlamydia trachomatis in cycloheximide-treated McCoy cells. J Clin Microbiol6: 329–31, 1977.
Mantel N, Haenszel W. Statistical Aspects of the Analysis of Data From Retrospective Studies of Disease. J Nat Cancer Inst22: 719–48, 1959.
Cox DR: The Analysis of Binary Data. London: Chapman and Hill Press, 1970, P. 87.
Svennson L, Westrom L, Mårdh P-A.Chlamydia trachomatis in women attending a gynecological outpatients clinic with lower genital tract infection. Br J Vener Dis57: 259–62, 1981.
Taylor-Robinson D, Tuffrey M, Falder P. Some aspects of animal models forChlamydia trachomatis genital infection. In Mårdh P-A, Holmes KK, Oriel JD, et al. (Eds.) Chlamydial Infections. Amsterdam: Elsevier Biomedical Press, 1982. Pp. 375–8.
Stamm WE, Holmes KK:Chlamydia trachomatis infections of the adult. In Holmes KK, Mårdh P-A, Sparling PF, Wiesner PH (Eds.) Sexually Transmitted Diseases. New York: McGraw Hill Press, 1984. Pp. 258–70.
Hobson D, Karayiannis P, Byng RE, et al. Quantitative aspects of chlamydial infection of the cervix. Br J Vener Dis56: 156–62, 1980.
Author information
Authors and Affiliations
Additional information
All authors are from the New York State Department of Health. Yangsook Han is a research scientist, AIDS Institute; Dale Morse is Director of the Bureau of Communicable Disease Control, Charles Lawrence is chief of the Biometrics Laboratory, Wadsworth Center for Laboratories and Research; Dennis Murphy is STD program director and Sally Hipp is STD special projects director.
Rights and permissions
About this article
Cite this article
Han, Y., Morse, D.L., Lawrence, C.E. et al. Risk profile forchlamydia infection in women from public health clinics in New York State. J Community Health 18, 1–9 (1993). https://doi.org/10.1007/BF01321516
Issue Date:
DOI: https://doi.org/10.1007/BF01321516