
Abstract
Purpose: We describe how the science of analyzing patient arrival and discharge data can be used to determine the optimal number of staffed OB beds to minimize labour costs.
Methods: The number of staffed beds represents a balance between having as few staffed beds as possible to care properly for parturientsvs having enough capacity to assure available staff for new admissions. The times of admission and discharge of patients from the OB unit can be used to calculate an average census. From this average census, and the properties of the Poisson distribution, the optimal number of staffed beds can be estimated. This calculation requires specification of the risk of having all in-house and on-call staff caring for patients, such that additional staff are unavailable should another parturient arrive. As an example, patient admission and discharge times were obtained for 777 successive patients cared for at an obstetrical unit. The numbers of patients present in the OB unit each two-hour period were calculated and analyzed statistically.
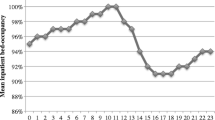
Principal findings: There was variation in the average census among hours of the day and days of the week. Poisson distributions fit the data for each of four periods throughout the week. Simply benchmarking the current average occupancy and comparing it to a desired occupancy would have been inadequate as this neglected consideration of the risk of being unable to appropriately care for an additional patient.
Conclusions: The optimal number of beds and occupancy of an OB unit to minimize staffing costs can be determined using straightforward statistical methods.
Résumé
Objectif: Montrer comment l’analyse des données sur l’arrivée et le départ des patientes peut servir à déterminer le nombre optimal de lits à assigner en obstétrique (OB) en vue de réduire le coût du travail.
Méthode: Le nombre de lits attribués représente un équilibre entre le fait d’avoir le moins de lits possibles pour pouvoir répondre aux besoins des patientes,vs avoir suffisamment de personnel disponible pour de nouvelles patientes. On peut utiliser l’heure d’arrivée et de départ pour le calcul du temps moyen passé en OB. À partir de ce séjour moyen, et des propriétés de la distribution de Poisson, le nombre optimal de lits réservés à l’OB peut être estimé. Ce calcul requiert la spécification du risque d’avoir tout le personnel sur place, en plus du personnel sur appel, affecté aux patientes, de sorte que personne ne sera disponible si une autre patiente se présente. Ainsi, les heures d’admission et de congé ont été obtenues pour 777 patientes successives admises à l’unité obstétricale. Le nombre de patientes présentes à l’unité OB à chaque heure a été soumis à un calcul et à une analyse statistiques.
Constatations principales: Le nombre moyen variait selon l’heure du jour et le jour de la semaine. Les distributions de Poisson s’accordaient aux données de chacune des quatre périodes de la semaine. Utiliser le temps moyen d’occupation courante comme référence et le comparer à l’occupation souhaitée serait inadéquat, puisqu’on ne tiendrait pas compte du risque de ne pouvoir assurer un traitement approprié à toute patiente supplémentaire.
Conclusion: On peut, dans le but de réduire le couût du personnel, déterminer le nombre optimal de lits et le meilleur taux d’occupation d’une unité d’OB à l’aide de méthodes statistiques simples.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Cormack RS. Predicting the obstetric work-load. Anaesthesia 1984; 39: 552–3.
Shonick W. A stochastic model for occupancy-related random variables in general-acute hospitals. J A S A 1970; 65: 1474–500.
Blumberg MS. “DPF concept” helps predict bed needs. Mod Hosp 1961; 97: 75–81.
Huang X-M A planning model for requirement of emergency beds. IMA J Math Appl Med Biol 1995; 12: 345–53.
Western Wisconsin Health Systems Agency Hospital Bed Need Task Force Final Report. 1981 Mar. 77. Sponsored by Bureau of Health Planning, Hyattsville, MD.
Thompson JB, Avant OW, Spiker ED. How queuing theory works for the hospital. Mod Hosp 1960; 94: 75–8.
Pike MC, Proctor DM, Wyllie JM. Analysis of admissions to a casualty ward. Br J Prev Soc Med 1963; 17: 172–6.
Thompson JD, Fetter RB. The economics of the maternity service. Yale J Biol Med 1963; 36: 91–103.
Vassilacopoulos G A simulation model for bed allocation to hospital inpatient departments. Simulation 1985; 45: 233–41.
McClain JO. A model for regional obstetric bed planning. Health Serv Res 1978; 12: 378–94.
Gupta T. Use of simulation technique in maternity care analysis. Computers Ind Eng 1991; 21: 489–93.
Wang ZJ, Avard D, Abernathy T, Nimrod C Birth patterns: are the Chinese in Guangzhou City different? Int J Gynecol Obtet 1988; 27: 25–35.
Ventura SJ, Martin JA, Curtin SC, Mathews TJ. Report of final natality statistics, 1995. Monthly vital statistics report. Hyattsville, Maryland: National Center for Health Statistics 1997; 45(Suppl 11): 39.
Lamiell MM. Modeling intensive care unit census. Military Med 1995; 160: 227–32.
Young JP. Administrative control of multiple-channel queuing systems with parallel input streams. Oper Res 1966; 14: 145–56.
Young JP. Stabilization of inpatient bed occupancy through control of admissions. Hospitals 1965; 39: 41–8.
Buffa ES, Cosgrove MJ, Luce BJ. An integrated work shift scheduling system. Decision Sci 1976; 7: 620–30.
Jenkin-Cappiello E. Oh babyl a labor and delivery staffing system measures patient census and acuity. Nurs Manage 2000; 31: 35–7.
Author information
Authors and Affiliations
Corresponding author
Additional information
Financial disclosure: Franklin Dexter is employed by the University of Iowa, in part as a consultant to anesthesia groups, companies, and hospitals.
Rights and permissions
About this article
Cite this article
Dexter, F., Macario, A. Optimal number of beds and occupancy to minimize staffing costs in an obstetrical unit?. Can J Anesth 48, 295–301 (2001). https://doi.org/10.1007/BF03019762
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03019762