
Abstract
Purpose: To compare the extent of the sensory, motor and sympathetic block produced by a single dose of 60 mg lidocaine at the same concentration (2%) and volume but at different baricity injected intraspinally.
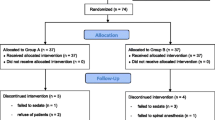
Method: In a randomised double blind study, 40 ASA I – II patients were scheduled for elective surgery (orthopedic, urologic, peripheral vascular and lower digestive procedure). They were divided in two groups. Twenty patients received 60 mg lidocaine 2% in a hyperbaric solution and 20 received 60 mg lidocaine 2% in a isobaric solution. The levels of sensory (pinprick, ice) motor (Bromage scale) and sympathetic blockade (galvanometry, cutaneous blood flow, temperature) were measured at 0, 5, 10, 15, 20 and 30 min.
Results: There were no differences between the groups with regard to maximal height of sympathetic block, sensory level to pinprick: T5±2.4 for isobaric group, T6±3.6 for hyperbaric group or to cold: T3±2.3 for isobaric group, T4±2.7 for hyperbaric group. Hyperbaric lidocaine 2% produced a more pronounced sensory (pinprick, ice) and motor block on the dependant than on the non-dependant side.
Conclusion: The baricity of 60 mg lidocaine injected intraspinally in the lateral decubitus position did not influence the cephalad spread of sensory or sympathethic blockade. In the hyperbaric group, the dependent side showed a more pronounced sensory (pinprick, ice), and motor block.
Résumé
Objectif: Comparer l’étendue du bloc sensitif, moteur et sympathique d’une dose de 60 mg de lidocaïne 2% à baricité différente, administrée en injection intrarachidienne, en décubitus latéral.
Méthode: Quarante patients ASA I–II, dont l’opération était prévue, ont participé à une étude randomisée à double insu. Ils ont été répartis aléatoirement en deux groupes. Vingt patients ont reçu une anesthésie rachidienne avec 60 mg de lidocaïne isobare à 2 %, et 20 patients avec 60 mg de lidocaïne hyperbare à 2%. Ont été mesurés sur une période de 30 min (0, 5, 10, 20, 30 min): l’expansion du bloc sympathique (galvanométrie, étude du flot vasculaire — Doppler — et prise de température aux extrémités), du bloc sensitif (aiguille et glace, côtés gauche et droit) ainsi que l’intensité du bloc moteur (gauche et droit). Une différence statistique deP<0,05 était considérée significative.
Résultats: Nous n’avons trouvé aucune différence significative intergroupe de diffusion céphalique de la sensibilité au froid et à l’aiguille. Les variations de température, de flot vasculaire, et de résistance cutanée étaient également comparables. Le bloc moteur était complet en 15 min chez tous les patients du groupe isobare, tandis que quelques patients n’avaient qu’un bloc partiel à droite (côté non dépendant) dans le groupe hyperbare, et ce, après 30 min.
Conclusion: La baricité d’une solution de 60 mg de lidocaïne 2% intrarachidienne n’influence pas le niveau céphalique sympathique, sensitif ou moteur en décubitus latéral. Cependant, un effet moteur plus marqué du côté déclive se dégage dans le groupe hyperbare.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Brown DT, Wildsmith JAW, Covino BG, Scott DB. Effect of baricity on spinal anaesthesia with amethocaine. Br J Anaesth 1980; 52: 589–96.
Bannister J, McClure JH, Wildsmith JAW. Effect of glucose concentration on the intrathecal spread of 0.5% bupivacaine. Br J Anaesth 1990; 64: 232–4.
Chambers WA, Edstrom HH, Scott DB. Effect of baricity on spinal anaesthesia with bupivacaine. Br J Anaesth 1981; 53: 279–82.
Vichitevejpaisal P, Svastdi-Xuto O, Udompunturux S. A comparative study of isobaric and hyperbaric solution of bupivacaine for spinal anaesthesia in Caesarean section. J Med Assoc Thai 1992; 75: 278–82.
Toft O, Bruun-Mogensen C, Kristensen J, Hole P. A comparison of glucose-free 2% lidocaine and hyperbaric 5% lidocaine for spinal anaesthesia. Acta Anaesthesiol Scand 1990; 34: 109–13.
Van Zundert AAJ, Grouls RJE, Korsten HHM, Lambert DH. Spinal anesthesia. Volume or concentration — what matters. Reg Anesth 1996; 21: 112–8.
Lui ACP, Munhall RJ, Winnie AP, Selander D. Baricity and the distribution of lidocaine in a spinal canal model. Can J Anaesth 1991; 36: 522–6.
Liu S, Pollock JE, Mulroy MF, Allen HW, Neal JM, Carpenter RL. Comparison of 5% with dextrose, 1.5% with dextrose, and 1.5% dextrose-free lidocaine solutions for spinal anesthesia in human volunteers. Anesth Analg 1995; 81: 697–702.
Bengtsson M, Malmqvist LA, Edström HH. Spinal analgesia with glucose-free bupivacaine — effects of volume and concentration. Acta Anaesthesiol Scand 1984; 28: 583–6.
Urmey WF, Stanton J, Bassin P, Sharrock NE. The direction of the Whitacre needle aperture affects the extent and duration of isobaric spinal anesthesia. Anesth Analg 1997; 84: 337–41.
Schawagmeier R, Schmidt A, Nolte H. The effect of injection speed and needle gauge on the spread of sensory blockade in spinal anesthesia. (German) Reg Anaesth 1990; 13: 148–52.
Casati A, Fanelli G, Cappelleri G, et al. Effects of spinal needle type on lateral distribution of 0.5% hyperbaric bupivacaine. Anesth Analg 1998; 87: 355–9.
Cohen J. Statistical Power Analysis for the Behavioral Sciences. New York, Academic Press, 1988.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jankowska, A., Veillette, Y. Comparison of differential blockade during spinal anesthesia using isobaricvs hyperbaric lidocaine 2%. Can J Anaesth 47, 137–142 (2000). https://doi.org/10.1007/BF03018849
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03018849