
Abstract
Purpose
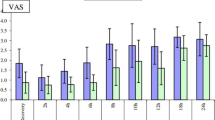
To compare the postoperative analgesic efficacy and safety of intrathecal (IT) néostigmine and IT morphine in patients undergoing total knee replacement under spinal anesthesia. Methods: Sixty patients scheduled for elective total knee replacement under spinal anesthesia were randomly divided into three equal groups which received IT 0.5% hyperbaric bupivacaine 15 mg with either normal saline 0.5 ml_, néostigmine 50 μg, or morphine 300μg. The maximal level of sensory block, duration of analgesia, time to use of rescue analgesics, the overall 24-hr and four-hour interval visual analogue scale (VAS) pain score, and the incidence of adverse effects were recorded for 24 hr after administration.
Results
There was no significant difference in maximal level of sensory block among the three groups. The morphine group had a later onset of postsurgical pain and longer time to first rescue analgesics than the néostigmine group (P < 0.05). Overall 24-hr VAS pain scores were significantly higher in the saline groupvs the morphine and néostigmine groups (P < 0.05). Motor block lasted significantly longer in the néostigmine group than in the morphine and saline groups (P < 0.05). The incidence of adverse effects was similar in the néostigmine and morphine groups except for pruritus (70%) occurring more frequently in the morphine group than in the néostigmine and saline groups (0%; P < 0.05). Overall satisfaction rates were better in the néostigmine group than in the morphine and saline groups (P < 0.05).
Conclusions
IT néostigmine 50 μg produced postoperative analgesia lasting about seven hours with fewer side effects and better satisfaction ratings than IT morphine 300 μg.
Résumé
Objectif
Comparer l’efficacité et l’innocuité analgésique postopératoire de l’administration intrathécale (IT) de néostigmine et de morphine chez des patients devant subir une arthroplastie totale du genou sous rachianesthésie.
Méthode
Soixante patients devant recevoir une prothèse totale de genou sous rachianesthésie ont été répartis au hasard en trois groupes égaux. Ils ont reçu 15 mg de bupivacaine hyperbare IT à 0,5 % et, soit 0,5 mL de solution salée, soit 50 μg de néostigmine, soit 300 μg de morphine. Le niveau maximal du bloc sensitif, la durée de l’analgésie, l’heure des premières demandes d’analgésiques de secours, les scores de douleur des 24 h d’observation et de chaque intervalle de quatre heures selon l’échelle visuelle analogique (EVA) et l’incidence d’effets indésirables ont été enregistrés pendant 24 h après l’administration médicamenteuse.
Résultats
Le niveau maximal de blocage sensitif n’a pas présenté de différence intergroupe significative. Chez les patients avec morphine, la douleur post-chirurgicale s’est installée plus tard et leur première demande d’analgésie de secours a donc eu lieu plus tard que chez les patients avec néostigmine (P < 0,05). Les scores de douleur à l’EVA ont été, sur 24 h, signifcativement plus élevés avec la solution salée vs la morphine ou la néostigmine (P < 0,05). La durée du blocage moteur a été signifcativement plus longue avec la néostigmine qu’avec la morphine ou la solution salée (P < 0,05). L’incidence d’effets indésirables a été similaire avec la néostigmine et la morphine, sauf pour le prurit (70%) qui a été plus fréquent avec la morphine qu’avec la néostigmine ou la solution salée (0 %; P < 0,05). Le taux de satisfaction générale a été meilleur avec la néostigmine qu’avec la morphine ou la solution salée (P < 0,05).
Article PDF
Similar content being viewed by others


References
Serpell MG, Millar FA, Thomson MF. Comparison of lumbar plexus block versus conventional opioid analgesia after total knee replacement. Anaesthesia 1991; 46: 275–7.
Singelyn FJ, Deyaert M, Joris D, Pendeville E, Gouverneur JM. Effects of intravenous patient-controlled analgesia with morphine, continuous epidural analgesia, and continuous three-in-one block on postoperative pain and knee rehabilitation after unilateral total knee arthroplasty. Anesth Analg 1998; 87: 88–92.
Gwirtz KH, Young JV, Byers RS, et al. The safety and efficacy of intrathecal opioid analgesia for acute postoperative pain: seven years’ experience with 5969 surgical patients at Indiana university hospital. Anesth Analg 1999; 88: 599–604.
Swart M, Sewell J, Thomas D. Intrathecal morphine for caesarean section: an assessment of pain relief, satisfaction, and side-effects. Anaesthesia 1997; 52: 373–7.
Stoelting RK. Intrathecal morphine — an underused combination for postoperative pain management. Anesth Analg 1989; 68: 707–9.
Eisenach JC, Hood DD, Curry R. Phase I human safety assessment of intrathecal neostigmine containing methyl and propylparabens. Anesth Analg 1997; 85: 842–6.
Hood DD, Eisenach JC, Tuttle R. Phase I safety assessment of intrathecal neostigmine methylsulfate in humans. Anesthesiology 1995; 82: 331–43.
Lauretti GR, Reis MP, Prado WA, Klamt JG. Doseresponse study of intrathecal morphine versus intrathecal neostigmine, their combination, or placebo for postoperative analgesia in patients undergoing anterior and posterior vaginoplasty. Anesth Analg 1996; 82: 1182–7.
Krukowski JA, Hood DD, Eisenach JC, Mallak KA, Parker RL. Intrathecal neostigmine for post-cesarean section analgesia: dose response. Anesth Analg 1997; 84: 1269–75.
Liu SS, Hodgson PS, Moore JM, Trautman WJ, Burkhead DL. Dose-response effects of spinal neostigmine added to bupivacaine spinal anesthesia in volunteers. Anesthesiology 1999; 90: 710–7.
Naguib M, Taksh TL. Characterization of muscarinic receptor subtypes that mediate antinociception in the rat spinal cord. Anesth Analg 1997; 85: 847–53.
Taksh TL, Grafe MR, Malkmus S, Rathbun ML, Eisenach JC. Studies on the safety of chronically administered intrathecal neostigmine methylsulfate in rats and dogs. Anesthesiology 1995; 82: 412–27.
Hood DD, Eisenach JC, Tong C, Tommasi E, Yaksh TL. Cardiorespiratory and spinal cord blood flow effects of intrathecal neostigmine methylsulfate, clonidine, and their combination in sheep. Anesthesiology 1995; 82: 428–35.
Gürün MS, Leinbach R, Moore L, Lee C-S, Owen MD, Eisenach JC. Studies on the safety of glucose and paraben-containing neostigmine for intrathecal administration. Anesth Analg 1997; 85: 317–23.
Slappendel R, Weber EWG, Dirksen R, Gielen MJM, van Limbeek J. Optimization of the dose of intrathecal morphine in total hip surgery: a dose-finding study. Anesth Analg 1999; 88: 822–6.
Chadwick HS, Ready LB. Intrathecal and epidural morphine sulfate for postcesarean analgesia — a clinical comparison. Anesthesiology 1988; 68: 925–9.
Morgan M. The rational use of intrathecal and extradural opioids. Br J Anaesth 1989; 63: 165–88.
Lauretti GR, Mattos AL, Reis MP, Prado WA. Intrathecal neostigmine for postoperative analgesia after orthopedic surgery. J Clin Anesth 1997; 9: 473–7.
Lauretti GR, Reis MP, Lima LCPR. Association of intrathecal fentanyl and intrathecal neostigmine: an effective postoperative analgesic for abdominal histerectomy. Reg Anesth 1996; 21(2S): 77 (abstract).
Tan P-H, Kuo J-H, Liu K, Hung C-C, Tsai T-C, Deng T-Y. Efficacy of intrathecal neostigmine for the relief of postinguinal herniorrhaphy pain. Acta Anaesthesiol Scand 2000; 44: 1056–60.
Chaney MA. Side effects of intrathecal and epidural opioids. Can J Anaesth 1995; 42: 891–903.
Alhashemi JA, Crosby ET, Grodecki W, Duffy PJ, Hull KA, Gallant C. Treatment of intrathecal morphineinduced pruritus following caesarean section. Can J Anaesth 1997; 44: 1060–5.
Author information
Authors and Affiliations
Corresponding author
Additional information
Research funding received from VGHKS 88-03, Veterans General Hospital-Kaohsiung, Taiwan, Republic of China.
Rights and permissions
About this article
Cite this article
Tan, PH., Chia, YY., Lo, Y. et al. Intrathecal bupivacaine with morphine or neostigmine for postoperative analgesia after total knee replacement surgery. Can J Anesth 48, 551–556 (2001). https://doi.org/10.1007/BF03016831
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03016831