
Abstract
Diagnostic radiologic image analysis or interpretation is a critical stage in the diagnostic process for the assessment of any pathologic condition (Table 15.1). The role of imaging in this sequence is to: (1) assist and/or confirm a suspected diagnosis, (2) provide direction towards the appropriate management of the condition, (3) identify surgical parameters of importance (e.g., pathologic margins, involvement of important anatomical structures such as the inferior alveolar canal), and (4) determine the effectiveness of a specific management strategy treatments with periodic assessment (postoperative follow-up radiographic examinations.
Similar content being viewed by others


Keywords
- Medication-related Osteonecrosis Of The Jaw (MRONJ)
- Keratocystic Odontogenic Tumor (KCOT)
- CBCT Images
- Osseous Dysplasia (OD)
- Radicular Cyst
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Fundamental Concepts in Diagnostic Radiologic Image Analysis
Diagnostic radiologic image analysis or interpretation is a critical stage in the diagnostic process for the assessment of any pathologic condition (Table 15.1). The role of imaging in this sequence is to: (1) assist and/or confirm a suspected diagnosis, (2) provide direction towards the appropriate management of the condition, (3) identify surgical parameters of importance (e.g., pathologic margins, involvement of important anatomical structures such as the inferior alveolar canal), and (4) determine the effectiveness of a specific management strategy treatments with periodic assessment (postoperative follow-up radiographic examinations.
Accurate and consistent radiologic interpretation and development of a differential diagnosis requires:
-
Images of diagnostic quality.
-
Comprehensive working knowledge of osseous and soft tissue anatomy and correlative radiographic anatomy.
-
An understanding of the basic nature and variability of the pathological process that affect the tissues maxillofacial region.
-
The formulation of a differential radiologic diagnosis with the disease entities arranged in decreasing order of probability, determined by the strength of their supporting evidence.
A diagnosis of an osseous disease can rarely be rendered from radiographic appearance alone a so-called “pathognomonic” presentation—however the radiologic appearance can provide important clues as to the nature of the disease.
Cone beam CT with its multi-planar (MPR) imaging capabilities provides an enhanced approach to radiologic maxillofacial diagnosis because of its three-dimensional or multidirectional visualization of the diseased tissues.
Diseases are classified according to the nature of the process or the tissue involved. Bony lesions can therefore be classified based on etiology (pathologic or surgical) (Table 15.2) or tissue of origin (Table 15.3). However, it is difficult to use this scheme in actually arriving at a list of possible diagnoses based on imaging presentation. Much of this process involves the use of historical, clinical, surgical, and histopathologic information to arrive at a differential diagnosis. Imaging is sometimes used to merely provide information about the location and extent of the disease.
1.1 Role of CBCT
The advent of CBCT has significantly added to the diagnostic efficiency and accuracy of dental diagnostic imaging and had a positive impact on treatment outcomes. This becomes self-evident for many diagnostic tasks including surgical planning, placement of dental implants, detection of apical pathoses, etc. In these situations, diseased tissue effects on known anatomical areas and boundaries as well as adjacent structures are clearly depicted by CBCT. Previously available two-dimensional dental imaging (periapical, panoramic, and cephalometric radiography) provided limited opportunities for extracting meaningful interpretive information and developing a diagnostic solution. This is because of inherent two-dimensional (2D) limitations such as the inability to observe cross-section changes, geometric distortion and overlapping of the disease process with neighboring, dense anatomical structures, referred to as anatomical noise. The transition from projection-based to office-based dental and maxillofacial CBCT imaging is arguably the single-most important contribution of radiography to diagnostic efficiency and improved treatment outcomes, especially in surgery. Indeed, the ability to view and examine an area of concern or a potential surgical site in three-dimensions (3D) has provided several more pieces of information to the interpretive puzzle of diagnosis. Although conventional radiography is often the primary modality for initial detection and identification of entities affecting the face and jaws, CBCT involves three-dimensional acquisition providing volumetric and multi-planar display leading to accurate representation of the following:
-
Lesional extent
-
Involvement of adjacent anatomic structures
-
Lesional borders
-
Internal lesional details such as septae and peripheral crenations
-
Presence and degree of root resorption, particularly on the buccal or lingual/palatal aspects of the lesion or tooth, respectively
Identification of many of these characteristics could potentially influence the differential diagnosis. For example, the presence of root resorption in association with a multilocular lesion is highly suggestive of neoplastic lesions, such as ameloblastomas and keratocystic odontogenic tumor (KCOT) (MacDonald 2011).
CBCT is very sensitive (91%) in the detection of invasion of adjacent bone by carcinoma, second only to that of MRI (94%) with specificity (100%) equal with both MRI and multi-detector CT (Uribe et al. 2013). Nevertheless, lesions whose clinical and/or conventional radiological presentations are suggestive of either a malignancy or vascular anomaly are more appropriately imaged by multi-detector CT (MDCT) with or without contrast, MRI or both. The superior contrast resolution of the latter imaging modalities better display invasion (malignant lesions) or involvement (vascular anomalies) of adjacent structures. CBCT is also limited if larger benign lesions (e.g., ameloblastoma and KCOT) perforate cortical borders or involve adjacent soft tissues (e.g., osteomyelitis). CBCT is optimal for benign pathology due to better spatial resolution, availability, and lower financial and radiation dose cost.
1.2 Considerations Prior to Diagnostic Image Analysis
-
Is a CBCT scan necessary and, if so, what kind of a scan? Cone beam CT is an optimal imaging modality for hard tissue assessment and should be prescribed when suspected disease involves in the osseous structures and/or teeth. The role of CBCT in soft tissue evaluation is limited to specific circumstances, such as the identification of the presence of luminal opacification in the paranasal sinuses and airway obstruction. A thorough clinical examination and review of available radiologic images is important to determine if a CBCT scan is needed by answering the clinical question, “Will the additional information gained add to the diagnosis?” If the answer to this initial question is “Yes,” then the second question is “What kind of a scan should be performed?” The answer to this question will provide guidance on the appropriate CBCT imaging protocol to be chosen.
Imaging protocol is determined by specific diagnostic concerns and results in developing task-specific imaging protocols—selection of available exposure and scanning parameters appropriate to the presenting situation. The imaging protocol includes the field of view (FOV) and the voxel resolution. The size of the pathological entity under investigation and the extent of the affected region will dictate the FOV to be selected (Scarfe and Farman 2008). Most CBCT scanners provide an adjustable FOV ranging from a projection area of exposure as small as 40 mm × 40 mm, appropriate for examining two to three teeth and their surrounding structures, to 150 mm × 150 mm, large enough to examine a large portion of the patient’s head (see Chap. 3). Extended or large FOV is appropriate for facial asymmetries, large developmental defects, and facial trauma whereas a smaller FOV is appropriate for edentulous sites for implant site assessment, single tooth impactions, endodontics, tooth defects, and periapical pathology (MacDonald 2017). Moreover, current CBCT scanners can acquire volumetric data with a voxel size between 0.08 and 0.4 mm nominal voxel resolution, which provide images with exceptional detail for hard tissue evaluation. Diagnostic tasks requiring high detail such as periapical pathology, missed and calcified canals external and internal root resorption, ankylosis, and root fractures almost always mandate choice of a small voxel resolution to achieve the needed image resolution.
CBCT scans, as well as other radiographic procedures, are also performed to assess the progression of disease or the outcome of a certain treatment or surgery (follow-up). The frequency of the follow-up examinations should be based on the suspected rate of the disease progression; certain pathological entities advance faster than others and no set rule exists as to the periodicity of these examinations. The follow-up clinical examination will determine how frequently scans should be acquired. Postsurgical follow-up or posttreatment scans are prescribed to assess the progress of treatment or surgery or healing. Osseous tissue healing is slow and these scans may be acquired every 6–12 months; they also may be substituted with simpler diagnostic images (e.g., panoramic or periapical radiography) if the clinician is satisfied by the progress of tissue healing. As always, the need for follow-up imaging and the selection of the appropriate type of imaging is determined after a clinical examination indicates that such an evaluation may be helpful. Progress of the treatment rendered is judged by comparing the follow-up radiographic examinations made at different time intervals after treatment or surgery with the initial radiographic examination.
While the above parameters provide some guidance on imaging procedures, a great deal of flexibility exists in the selection of the proper CBCT imaging protocol. The optimal protocol should ultimately be based on the clinician’s judgment, knowledge, and professional responsibility, with the clinical examination as the deciding factor.
-
Is the acquired scan of diagnostic quality? Poor image quality may obscure important details especially more subtle or early changes in the site under examination and this may compromise diagnosis. The association between high image quality and diagnostic efficiency is well established in the literature (White and Pharoah 2009).
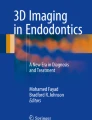
The most frequent factors affecting image quality of a CBCT scan are patient motion during the scan acquisition and artifacts. Despite the fast acquisition time of CBCT scanners, patient motion may occur during the scan and may have a detrimental effect in image quality. Strict adherence to the manufacturer’s recommendations on patient positioning and head stabilization in the scanner may reduce the likelihood of motion. A thorough review of the entire volumetric data immediately after the procedure—while the patient still is present—should be performed to identify signs of patient motion within the image. If there is evidence of patient motion, such as blurred images or double margins, that is likely to obscure diagnosis, the procedure should be repeated (Fig. 15.1).
The presence of artifacts in the CBCT scans may have an effect on image quality and diagnostic efficacy (Bechara et al. 2012). Metallic restorations are the most frequent cause of artifacts. They present with alternating bright and dark bands or a “sunray” appearance and may make it impossible to evaluate any areas of the scan that may overlap with the region of interest. They are most often present at the level of the crowns of the teeth and may have a detrimental effect especially in fine diagnostic tasks like the detection of crown and root fractures, early periodontal defects, and other defects adjacent to metallic restorations. Under these circumstances, a clinician’s knowledge and experience will assist develop realistic expectations about the diagnostic efficiency of this exciting imaging modality.
-
What kind of image reconstructions should be applied? Appropriate image reconstructions must provide a complete evaluation of the anatomical region of interest and address a specific diagnostic concern. MPR and interactive software applications offer tremendous opportunities for the clinician to unlock the diagnostic capabilities of CBCT. Application of specific reformatting options should be directed towards extracting the maximum diagnostic information. This demands a methodological approach and knowledge of the utility of specific reformatting methods.
-
Appreciate the limitations of CBCT Imaging. While the inherent high spatial resolution of CBCT imaging demonstrates osseous anatomy accurately, there are specific diagnostic tasks for which CBCT is not suited because of low contrast resolution. These include the following:
-
Differentiation of the intralesional contents (e.g., fluid vs. tumor)
-
Lesional extension through cortical perforation
-
Adjacent soft tissue reaction (e.g., cellulitis associated with osteomyelitis)
-
Intra-articular disorders (e.g., temporomandibular disc position, synovitis)
-

Screen capture of a temporomandibular joint software display showing coronal sections of the right and left TMJ on either side of an axial section at the level of the condyles (above). These images are used for the reconstruction of a series of cross-sectional images of the right and left TMJs (below). All images show extensive patient motion artifacts that have compromised clarity of the mandibular condyles. The anatomical structures of interest are poorly visualized and the imaging procedure needs to be repeated
Overall and regional image quality can also be influenced by various factors including patient-related artifacts (Fig. 15.1) and inherent artifacts (e.g., radiolucent streaks and radiopaque scatter due to beam hardening).
2 Analysis of CBCT Images
Radiologic interpretation ascribes meaning to observations of imaging characteristics and results in the development of a differential diagnosis—a list of possible diagnoses, ranks in order, consistent with the radiologic and clinical findings. Interpretation involves a sequence of cognitive steps. The description of the imaging characteristics of a suspected pathology, identification of patterns of bony involvement and associated disease processes and subsequent categorization into groups providing a radiologic differential diagnosis is known as radiologic pattern recognition.
2.1 Collect All Available Diagnostic Information
The review of a CBCT scan is a step-by-step analysis of all abnormal radiographic findings or features with the goal of recognizing and collecting as much information as possible that is available in the various image reconstructions (White and Pharoah 2009). Described in detail earlier, the mechanics of radiologic analysis involves principally the methodological interactive display of the data set initially using orthogonal projections (i.e., axial, sagittal, and coronal) and then task-specific display protocols (e.g., reformatted panoramic and associated trans-axial images, volumetric rendering). Systematic review is necessary and requires multiple “sweeps” through the image sets focusing on different systems including:
-
Gnathic
-
Maxilla and maxillary teeth
-
Maxillary sinus
-
Mandible and mandibular teeth
-
Temporomandibular joint
-
-
Extra-gnathic
-
Nose and paranasal sinuses
-
Soft tissues of the neck
-
Cervical spine
-
Airway
-
Cranial vault
-
In reviewing each of the anatomical regions mentioned above, special attention should be paid to the “chief complaint” or the reason for the scan acquisition. The review may start from the region of concern, since one naturally is trying to identify “what’s wrong” first. This is a common practice in most, if not all, disciplines of medicine and dentistry including oral and maxillofacial radiology. Modifications to the algorithm described above may be necessary depending on a clinician’s individual approach.
2.2 Look for the Abnormality
A thorough review of the CBCT scan above should reveal the abnormality; this task may be guided by the reported patient history and the clinical findings. Key observation features that may indicate an abnormality include:
-
Changes in the appearance of known tissues and structures in the maxillofacial region. Most dental practitioners are well acquainted with the normal appearance of the osseous structures of the maxillofacial region (shape and size, anatomical boundaries and contours, etc.). Variations from normal patterns may be suspicious for developing abnormality or even pathology (Fig. 15.2).
-
Changes in the bone density. These are a frequent indicator of disease development. The most common localized alteration of the cancellous bone pattern is associated with periapical pathosis (Fig. 15.3).
-
Asymmetry in known bilateral structures. A deviation shape or form as compared to a contralateral structure is a sign of unilateral growth or atrophy and may indicate disease (Fig. 15.4). Differences between the right and left side in gross anatomical structures such as condylar heads, mandibular ramii, paranasal sinuses, and walls of the airway raise suspicion for abnormality as developing diseases tend to be unilateral. Anatomical variations tend to be bilateral. Anatomical variability between individuals and sometimes even within the same individual adds considerable difficulty in diagnosis. In these situations diagnosis may be assisted by viewing the radiologic abnormality in the light of clinical or historic findings.

Reformatted panoramic (a) and series of cross-sectional images (b) of the left mandible demonstrating homogenous high-density mandibular bone; the sclerotic cancellous bone is almost indistinguishable from the cortical bone. In addition, there are high-density sequestrations present in the left posterior mandible, adjacent to the alveolar crest. Together with the patient’s history of bisphosphonate therapy and long-term clinically exposed bone in this region, this imaging presentation is consistent with a diagnosis of medication-related osteonecrosis of the jaws (MRONJ)

A series of cross-sectional images in the left mandible showing an altered cancellous bone pattern. The mandibular cortices are thin with effacement of the internal margin and the trabeculae are sparce. The above findings are suspicious for osteoporosis

An axial (a) and coronal (b) image depicting marked asymmetry between the right and left maxillary sinuses with the left one being considerably smaller in size. This imaging appearance is consistent with left unilateral maxillary sinus hypoplasia. This is a developmental defect that requires no attention
2.3 Determine the Location of the Abnormality
Identifying the accurate location of the abnormality may be revealing as to the tissue or structure of origin or possible association with specific tissues. Most pathological entities in the maxillofacial region follow a domestic pattern: they develop and grow within the tissue from which they have originated. The only exceptions are metabolic conditions, systemic conditions, and metastatic disease. For example, if an intraosseous abnormality under assessment is located in tooth-bearing areas of the jaws, there is a high likelihood that it is of odontogenic origin (dental in origin) (Fig. 15.5). Similarly, if a lesion is located in a non-tooth-bearing area, there is a high likelihood that it is of non-odontogenic origin (Figs. 15.6 and 15.7). Tooth-bearing areas are the alveolar ridges in the maxilla and mandible. In the maxilla, the base of the alveolar bone is somewhat below the floor of the maxillary sinus and the floor of the nasal cavity. The mandibular alveolar bone is bordered by the mandibular canal in the posterior mandible and the mental ridge in the anterior mandible. These tooth-bearing zones (with the exception of the mandibular canal) are fairly vague and this may cause some confusion as to the accurate localization of a lesion. In these situations, additional determinants may be employed.

A reformatted panoramic (a) and series of cross-sectional images (b) depicting a well-defined, mixed-density, unilocular entity in the left retromolar trigone. The lesion contains several small, high-density foci which look like tooth structures or tissues. The location of the lesion in question is above the left mandibular canal (tooth-bearing region) and suggests the entity is of odontogenic origin. The most likely diagnosis is compound odontoma


Reformatted panoramic (a) and a series of cross-sectional images (b) depicting a well-defined, mixed density lesion in the left angle of the mandible. The entity is surrounded by an irregular and hyperostotic border and contains 2 to 3 high-density foci. The lesion is below the left mandibular canal (non-tooth-bearing region) which indicates a non-odontogenic origin (most likely). The imaging appearance is most consistent with a diagnosis of focal osseous dysplasia

Panoramic reformatted (a), axial reference (b) and cross-sectional (c) images of the left mandible showing a well-defined, semispherical defect in the lingual mandibular cortex in the molar region (green arrow). This defect extends to include the internal margin of the buccal cortex. The lesion is below the left mandibular canal (red arrow) which suggests a non-odontogenic origin. In this case, the imaging appearance and location are consistent with a lingual bone defect or Stafne bone cavity (anatomical variant)
The epicenter of the lesion may be of assistance in determining the tissue of origin (White and Pharoah 2009). If the epicenter of a lesion is inside the nasopalatine canal or inside the mandibular canal, the content of these canals should be linked to its origin (Figs. 15.8 and 15.9). If the epicenter of a lesion is inside the nasal cavity or the maxillary sinus, it is unlikely the lesion is of odontogenic origin. However if there is an osseous elevation arising from the floor of the maxillary sinus, this is suspicious of a lesion which has originated in the alveolar bone and is expanding superiorly (Fig. 15.10).

Axial (a) and sagittal (b) orthogonal images of the anterior maxilla showing a well-defined, round, low-density unilocularity in the midline of the alveolar ridge between the central incisors (green arrows). While close to a tooth-bearing region, the lesion originated from the nasopalatine canal which appears to be eroded. The imaging appearance is consistent with a diagnosis of a nasopalatine duct cyst (non-odontogenic) which has eroded the labial and palatal cortices as well as the floor of the nasal cavity (red arrows)

Reformatted panoramic (a) and a series of cross-sectional images (b) of the mandible depicting a well-defined, unilocular, hypodense entity which coincides with the left mandibular canal. The cross-sectional images clearly demonstrate that there is a gradual increase in diameter of the mandibular canal (red arrows). This suggests an origin inside the mandibular canal of possible vascular or neural (non-odontogenic) origin

A local reformatted panoramic (a) and series of cross-sectional images (b) of the right posterior maxillae depicting a well-defined, unilocular hypodense ovoid lesion in the apical region of the right second molar (red arrows). This has originated in the alveolar bone (apical pathology from pulpal necrosis) and as it progressed slowly, has caused an expansion of the floor of the right maxillary sinus. The green arrows show perforation of the maxillary sinus floor
2.4 Determine and Describe Key Features of the Abnormality
Radiographic images alone, including those produced with CBCT, are seldom conclusively diagnostic. History, physical examination, and biopsy are usually prerequisites to final diagnosis. The various pathological entities that may present radiographically in the maxillofacial region differ in appearance. Various characteristics provide insight into the nature, growth pattern, aggressiveness, and progression of the lesions. These features have been studied in depth and are listed in several textbooks; however, most descriptions refer to previous 2D dental imaging, specifically intraoral and panoramic images. This has been changing gradually, with the growing utilization of CBCT for routine dental diagnosis; the collective experience of CBCT use by the authors is presented in this chapter.
It is important to acknowledge that soft tissue pathological entities are impossible to distinguish from CBCT images because of the poor soft tissue contrast. Unless such soft tissue lesions affect the normal shape and size of known neighboring anatomical structures (airway, nasal cavity) or invade osseous structures, they likely will be unidentifiable in CBCT scans and will continue to grow silently unless diagnosed clinically or by other diagnostic methods.
However, a thorough and comprehensive analysis of the radiographic characteristics is an important tool in categorizing the general nature of hard tissue lesions (Table 15.4).
-
Degree of Attenuation. In multi-detector computed tomography (MDCT), the overall presentation of an entity is described related to changes in attenuation due to loss or gain of osseous material. Because of the similarities with MDCT images, the three (3) general presentations of a lesion on CBCT images are characterized using similar language; low density/attenuating, high density/attenuating, and mixed density/attenuating (demonstrating both low- and high-density features). Previously, in 2D maxillofacial imaging, the terms radiolucent, radiopaque, and radiomixed were used, respectively. These categories may show additional internal characteristics.
-
Shape and nature of the lesion’s borders. The shape and borders of a pathological entity will provide some suggestion as to its nature and even growth rate. Slow-growing pathological entities usually demonstrate a smooth border, whereas irregular borders often characterize more aggressive conditions. Cystic lesions usually are round or ovoid in shape within the constraints of the shape of the jaw in the region they have developed. The borders of a lesion require some special attention: They are characterized as “well defined,” “moderately defined,” or “poorly defined” based on how clear the distinction is between the affected and unaffected by the lesion tissues. Well-defined entities are those in which there is absolute certainty about the margin of the lesion, with a definite line separating the diseased from the healthy tissue. Often, there may be a thin, high-density (corticated) line which borders the lesion (Fig. 15.11). This feature is characteristic of a benign, slow-growing lesion and is commonly found in cysts. Larger cystic lesions may expand and thin bony cortices, and, on some occasions, may perforate them. In such cases, it is possible that the lesion communicates with the oral cavity and becomes contaminated. Contaminated cystic lesions frequently behave like abscesses and may lose their clear delineation (Fig. 15.12).
In other occasions, the border is thicker, described as “sclerotic” or “hyperostotic”: this is a feature of either very slow-growing lesions or reactive bone formation stimulated by the lesion like on chronic inflammation (Fig. 15.13). When there is no distinction between affected and unaffected osseous tissues, the border of these pathological entities is characterized as “poorly” defined (or ill-defined); in such cases, there is a gradual transition from the normal-appearing bone to the abnormal that it appears as if the border is blending (White and Pharoah 2009) This appearance is seen commonly in solid pathological entities which are generally benign like fibrous dysplasia (Fig. 15.14). Lesions that demonstrate invasive, erosive, or permeative borders are rather aggressive and may be associated with rapid growth and tissue destruction. This is a characteristic of malignant lesions. In these lesions, the progression is not through expansion, as in benign lesions, but via destruction at the expense of trabeculae (White and Pharoah 2009) (Fig. 15.15).
-
Distribution. The distribution of a pathologic entity can be described in relation to its association with the dentition (e.g., pericoronal, inter-radicular), jawbone, of intra- or extraosseous presentation, location within the jaws and number (Table 15.4).
-
Shape. Studying the shape of the deformity made by a pathological entity often contributes to developing a differential diagnostic list; in fact, a broad distinction between some categories of pathological entities may be made based on the internal structure (like the differentiation between a solid mass and a cystic lesion). Lesions that demonstrate a uniform, low-density content and a single chamber (unilocular) are often cystic lesions (Fig. 15.16).
Sometimes septae may divide the lesion into a series of smaller chambers called loculations. This appearance is referred to as multilocularity. Both solid benign tumors and some cysts may show multilocularity. The number of loculations and their shape and size are also of importance since they may characterize certain pathological entities; benign tumors show frequently a multilocular internal pattern (more frequently than cysts). For example, an ameloblastoma (Figs. 15.17 and 15.18) may present with larger loculations which resemble a “soap-bubble” appearance (Fig. 15.19) whereas lesions with smaller loculations are referred to as “honeycomb.”
-
Internal architecture. The basic descriptors of the internal architecture of a lesion include a consideration of the homogeneity of the entity, the presence of calcifications or septae, and alterations in trabecular pattern. Some patterns are associated with specific entities (Table 15.4). In some cases the overall appearance of a lesion may be cystic containing high-density flecks or one or more high-density cores inside the lumen of the lesion. Despite the distinction, these fall in the broader category of mixed lesions and are mostly benign tumors or rarely some types of cysts (Figs. 15.20 and 15.21). High-density or mixed density lesions may also show variations in their internal structure that may be significant. High-density entities may be due to the formation of abnormal osseous tissue; in fact, if the trabecular pattern of healthy bone is altered and replaced by denser, smaller trabeculae, this will increase the overall density of the affected site. A mixture of bundles of denser, smaller trabeculae interchanged with layers of normal, healthy ones may reflect a mixed internal structure (Fig. 15.22). In all instances, a high-density or mixed appearance in a lesion under investigation is a strong indication of a solid mass (Figs. 15.22, 15.23, and 15.24).
-
Response of the surrounding tissue to the presence of the lesion. The effects of the lesion on the surrounding tissues vary and will provide information about the behavior of the developing pathology. As they advance in size, slow-growing lesions gradually occupy more space and in that process will often displace teeth (Fig. 15.25), may cause root resorption (Fig. 15.26), may expand bony cortices, and, in general, may displace anatomic structures in the vicinity. These may include the floor of the maxillary sinuses and nasal cavities, if they grow in the maxilla (Fig. 15.27), or the mandibular canal and mental foramen (Fig. 15.28), if they are developing in the mandible. While this commonly is seen in large lesions, it may be seen even in smaller ones causing what is known as the “halo effect” (Fig. 15.29). These findings are often associated with benign pathological entities such as cysts or benign neoplasms.
Fast-growing lesions, especially malignancies and inflammatory lesions, will cause significant peripheral destruction of the tissues or structures adjacent to the lesion rather than cause displacement. The most characteristic imaging findings suggesting a malignancy or inflammatory process include:
-
Eroded or destroyed cortices.
-
“Floating teeth” (the destruction of the supporting bone has made the teeth in the region to look like they float) (Fig. 15.30).
-
Irregular widening or destruction of lamina dura.
-
Invasion and destruction of the mandibular bone and bony cortices.
-
Destruction of the walls of the mandibular canal and accompanying paresthesia (Fig. 15.31).
-
“Moth-eaten” destruction pattern or borders of the affected bone (Fig. 15.32).
-

Reformatted panoramic (a) and a series of cross-sectional images (b) of the mandible (B) depicting a well-defined, round, low-density, homogenous entity which is surrounded by a thin corticated border (red arrows). All features are characteristic of a benign, slow-growing lesion. Note the thinning of the labial cortical plate (yellow arrows) caused by the expanding cystic lesion. This lesion was associated with the apical region of the right mandibular canine and histologically confirmed as a radicular cyst

Reformatted panoramic (a) and a series of cross-sectional images (b) of the left anterior maxilla depicting a moderately defined, homogenous, low-density lesion in the apical region involving multiple teeth. The entity has resulted in thinning and possible erosion of the palatal cortical plate (red arrows) and, to a lesser extent, thinning of the labial cortical plate (yellow arrows). These features are suggestive with a radicular cyst communicating with the oral cavity. If a cystic lesion communicates with oral cavity, it may become infected and may behave like an abscess. Note the marked soft tissue intraoral expansion involving the hard palate (green arrows)

A series of CBCT cross-sectional images of the maxillary left canine showing a large, homogenous, low-density, trapezoidal-shaped, cystic lesion. The thick-hyperostotic border noted is the result of reactive bone formation associated with chronic inflammation. The red arrows show a communication through which the lesion drained in the oral cavity. The imaging appearance is consistent with a radiologic diagnosis of radicular cyst with an “abscess”-like behavior

A series of CBCT axial orthogonal sections showing marked asymmetry between the left and right posterior mandible. The left mandibular body shows marked expansion of the cortices and a “ground glass” appearance in an area the borders of which are not clearly determined (poorly defined lesion). The imaging findings are consistent with a diagnosis of fibrous dysplasia of the left mandible


Reformatted panoramic (a) and a series of cross-sectional images (b) of the left maxilla and mandible illustrating a large, ovoid, moderately defined, low-density lesion with rather irregular borders. Note the extensive destruction of the osseous tissues seen at the margins of the lesion (red arrows). Faint opacities seen within the lesion are most likely osseous remnants. These features are strongly suggestive of an aggressive, most likely malignant pathological entity. Also, note the destruction of the maxillary alveolar process (yellow arrows)

Cropped reformatted panoramic (a), para-coronal (b), and axial (c) images of the left mandible showing a well-defined, ovoid lesion of uniform low density with a corticated border. Note the marked expansion of the bony cortices and thinning of the lingual and inferior cortex. This appearance is characteristic of a cyst and consistent with a dentigerous cyst. However, some solid lesions also mimic this appearance including ameloblastoma and keratocystic odontogenic tumor (KCOT)

Reformatted panoramic (a) and a series of cross-sectional images (b) of the maxilla depicting a well-defined, homogenous, multilocular, low-density lesion associated with the apical region the anterior and right premolar teeth occupying almost the entire anterior maxilla (red arrows). This has caused marked expansion and thinning of the labial and palatal cortices (green arrows) and erosion of the cortices in some areas (yellow arrows). The radiologic appearance is suggestive of a solid benign tumor such as an ameloblastoma (final diagnosis) or keratocystic odontogenic tumor (KCOT)

Reformatted panoramic (a) axial (b), and a series of cross-sectional images(c) of the mandible (B) depicting an extensive, well-defined, multilocular, low-density lesion occupying almost the entire left posterior mandible. The loculations are small and the lesion shows a “soap-bubble” appearance. This has caused marked expansion and thinning of the buccal, lingual and inferior cortices. The imaging appearance is suggestive of ameloblastoma and keratocystic odontogenic tumor (histopathologic diagnosis)

Reformatted panoramic (a) and a series of cross-sectional images (b) depicting a moderately defined, expansile, multilocular mass in the anterior maxilla. Note that on the cross-sectional images (b) many of the trabecular are fine and angularly oriented demonstrating a “tennis racket” pattern with almost square loculations. The overall appearance is suggestive of benign tumor; the trabecular pattern may be associated with an odontogenic myxoma (histopathologic diagnosis)

Reformatted panoramic (a) and a series of cross-sectional images (b) depicting a well-defined, mixed attenuating lesion in the apical region of the right mandibular anterior teeth containing three to four small distinct globular hyperdensities with a hypodense periphery. The lesion has expanded and thinned the lingual mandibular cortex. These findings are suggestive of focal osseous dysplasia

Reformatted panoramic (a) and a series of cross-sectional images (b) of the mandible (B) depicting a single, well-defined, mixed attenuating lesion in the apical region of the right canine which contains high-density flecks (red arrows). The lesion has slightly expanded and thinned the labial and lingual mandibular cortex. In the absence of similar entities, these findings are suggestive of an ossifying fibroma

Axial (a), coronal (b), and midsagittal (c) sections of the anterior mandible depicting a moderately defined, expansile, mixed attenuating, solid mass which has markedly expanded the mandibular cortices. These findings are suggestive of a benign tumor; the resorptive replacement resorption of the apex of the roots of some of the incisor teeth is suggestive of osteoblastoma (histopathologic diagnosis)

Limited FOV CBCT image displays of two patients showing irregular, well-defined, homogenous, high-density lesions; one is in left posterior mandible resorbing or replacing the mesial root of the first molar and extending to almost the entire inferior mandibular cortex (red arrows) (a); the second hyperdensity is intraradicular and triangular in shape (red arrows), (b) apparently causing displacement of the roots of premolar teeth. The high-density appearance is an indication of a solid entity. The imaging appearance is consistent with idiopathic osteosclerosis in both cases

Axial (a), cross-sectional (b) and reformatted panoramic (c) image sections showing a round, well-defined, pedunculated hyperdense, exophytic entity originating from the inferior mandibular cortex just anterior to the left mandibular angle (non-tooth-bearing region). Internally the density is similar to that of bone with a cancellous and a cortical component. The imaging appearance is consistent with a mandibular osteoma

Panoramic reformatted (a) and cross-sectional images (b) of the anterior mandible (limited FOV) showing a well-defined, pear-shaped homogeneous hypodense lesion causing displacement of the anterior central incisors. Displacement of teeth is a common phenomenon associated with the slow enlargement of benign pathological entities; this lesion histopathologically proven to be a unicystic ameloblastoma

Reformatted panoramic (a) and a series of cross-sectional images (b) of the mandible showing a well-defined, ovoid, homogenous low-density entity in the anterior mandible with displacement and “knife-edge” root resorption on multiple incisor teeth (red arrows). These features are typical of benign pathological entities with the pattern of root resorption being highly suggestive of ameloblastoma (histopathologic diagnosis)

Reformatted panoramic (a) and cross-sectional image (b) of the maxillary left molars showing the effects of a slow-growing superiorly expanding radicular cyst raising the floor of the left maxillary sinus (arrows)

Reformatted panoramic (a) and series of cross-sectional images (b) illustrating the marked expansion effects of a large pericoronal unilocular ovoid hypodensity on the mandibular cortices and associated lingual displacement of the mandibular canal (red arrows)

Coronal (a) and parasagittal images (b) of the maxillary left premolars showing a elevation of the floor of the left maxillary sinus (arrows) immediately superior to the apex of the root of the second premolar caused by a local periapical inflammatory lesion; this is known as “halo effect,” a sign of slow-growing lesions

Sequential thin slice reformatted panoramic images of the mandible of 12-year-old boy showing marked permeative destruction of the cancellous component of the mandibular bone including loss of lamina dura and trabeculation. These features highly suggestive of a malignancy (histologically diagnosed as a Burkitt lymphoma)

Series of cross-sectional images (a) and a reformatted panoramic image (b) of the right posterior mandible illustrating the effects of poorly defined, aggressive lesion (red arrows) on the mandibular bone: Note the marked destruction in the cancellous component of the mandibular bone (showing as void in the cross-sections), destruction of the bony cortices (yellow arrows) and permeative signs (green arrows) as the lesion is invading the mandibular cortices. These are common features of aggressive or malignant pathological entities. The histopathologic diagnosis was osteomyelitis


Reformatted panoramic (a) and series of cross-sectional images (b) of the anterior mandible showing the characteristic “moth-eaten” pattern present on the lingual and inferior cortex. This feature is highly suggestive of an aggressive, invasive pathological entity. Correlated with moth the medical history (previous bisphosphonate use) and clinical presentation, the final diagnosis was medically related osteonecrosis of the jaw
Numerous schemes have been proposed incorporating radiologic features to assist clinicians as an aide–mémoire including:
-
L.E.S.I.O.N. (Gonzalez 2015): Acronym for lesion, edge, shape, internal, other structures, and number.
-
“Lazy dental students surely become increasingly stupid” Pneumonic for location, (radio) density, shape, size, borders, internal structure, surrounding tissues.
-
Five S’s and Three D’s (MacDonald 2011): Catch phrase for shade, shape, site, size, surroundings, diameter, density, and displacement.
Whichever scheme is used for radiologic data collection, the purpose of using radiographic descriptors (Table 15.4) suggestive of specific disease processes is to match the imaging findings to radiologic patterns.
2.5 Putting Everything Together
Once the imaging of an entity has been reviewed in detail and all key features identified, the significance of each characteristic must be determined so that the entity can be categorized into a specific radiologic pattern. Radiologic patterns of tissue involvement are based principally on degree of attenuation, tooth association, number of entities present, lesion shape, and location of the entity with respect to the tooth. Use of this algorithm (Fig. 15.33) provides a manageable list of conditions that present with these characteristics. Further differentiation within these groups is dependent on knowledge of specific disease-related imaging characteristics.

Simplified three- and four-tier radiologic pattern description algorithm based on level of attenuation, tooth association, location, number, and shape
In this process, the clinician must address the following considerations:
-
Is the suspected abnormality potentially a true pathological entity or an anatomical variant? A knowledge of the radiologic appearance of possible anatomical variants that may look suspicious or imitate disease is an important step in the diagnostic process. This requires a sound knowledge of the anatomy of the maxillofacial region. This understanding is not trivial as there are a wide range of anatomic variability in the maxillofacial region.
-
Is the abnormality localized or generalized? Generalized pathologic entities are usually the result of systemic, metabolic, or endocrine disorders; in this case the entire maxilla or mandible or more bones may be affected.
-
From where is the lesion originating (origin)? This requires a thought related to two aspects; “Is the entity potentially developmental or acquired?” and “From which tissue (bone or soft tissue) and anatomical area is the most likely the origin of the lesion?” Alterations in the radiographic appearance of the affected region, determination of the lesional epicenter, changes in adjacent anatomical structures, and indirect effects within the surrounding tissues may reveal information as to whether the entity has an osseous or soft tissue origin. In dental and maxillofacial imaging, primary radiologic categorization and subsequent differential diagnosis is based on determining if the entity is tooth-associated or non-tooth-associated (Tables 15.5 and 15.6).
-
Is this possibly a benign or a malignant lesion? Radiographic hallmarks of a malignancy include an irregular shape, evidence of fast growth, and an invasive and destructive behavior. In contrast, benign pathological entities such as cysts or benign tumors are slow growing and demonstrate round or ovoid-shaped well-defined lesions that displace and push the neighboring tissues instead of invading them (Table 15.7). The available clinical information may assist in determining possible metabolic, systemic, or inflammatory causality of a benign lesion.
-
Apart from the area of interest, is there anything else that should be reviewed? An important step towards the completion of the diagnostic process includes the thorough review of the entire imaging volume to ensure that no incidental or synchronous disease is inadvertently omitted from consideration.
-
Are there any radiographic features present that could be considered as highly suggestive of a particular disease or act as a “red flag”? Few pathological entities can be diagnosed from their radiographic features alone. In most cases, the clinician will formulate a list of possible diagnoses. Many entities are discovered serendipitously on an imaging examination usually performed for other purposes (e.g., assessment of third molars). Others may present as localized expansions. In formulating a differential diagnostic list, one should be aware of features and presentations that are highly suggestive of certain disease entities:
-
Symptomatic presentation such as pain, altered sensation (paresthesia) should always alert the clinician to neurovascular infiltration by either infections or malignancy until proved otherwise.
-
Cysts have a number of “cardinal” radiographic features that when considered together assist in their differential diagnosis (Fig. 15.34).
-
Specific areas of the jaw are associated with the development of specific conditions, particularly cysts (Fig. 15.35).
-
Some well-defined lesions present predominantly in children (ameloblastic fibroma, ameloblastic fibro-odontoma) or young adults (traumatic bone cavity, adenomatoid odontogenic tumor) while others occur more commonly in males (traumatic bone cavity, ameloblastic fibro-odontoma)
-

Imaging features suggestive of cyst pathology

Many solitary well-defined radiolucent lesions, especially cysts, tend to occur in specific areas. Traumatic bone cysts most frequently occur in the mandibular premolar area and extend between the apices of the teeth. Similarly, in the maxilla, incisive canal cysts only present in the incisive canal regions. The submandibular salivary gland developmental defect only presents coincident or below the mandibular canal
Often times, there might be a need for further investigation: this may be either with additional advanced imaging, biopsy, possible treatment, or periodic evaluation (White and Pharoah 2009). Some pathological entities may require immediate attention whereas for others periodic observation may be a more appropriate. Consulting a specialist in oral and maxillofacial radiology may provide guidance not only when there is difficulty in diagnosis but also in developing management strategies.
Finally formal documentation of all findings and notes of each reviewed CBCT volume provides an invaluable patient record for future use, enhances communication with other clinicians, and serves as a legal record. This will also provide documentation as to the progression of a pathological entity or the progress of certain treatments.
3 Key Considerations in Radiologic Presentation of Maxillofacial Pathology
3.1 Low-Density Lesions
The most common pathologic presentation for pathology in the jaw is that of a low-density lesion. While it is beyond the scope of this chapter to describe the clinical and distinctive radiographic features of radiolucent entities, they are numerous key points that should be appreciated.
-
The most frequent radiolucency of the jaws is of periapical inflammatory origin. Smaller periapical lesions are as a result of chronic apical periodontitis whereas larger entities most often appear as a single, well-defined, unilocular, homogenous, low-density lesion arising secondary to necrosis of the dental pulp due to caries (Figs. 15.36 and 15.37) or trauma. Histologically these entities could be a granuloma, radicular cyst or abscess. Rosenberg and co-authors (2010) reported that CBCT findings cannot reliably distinguish a granuloma from a cyst. Tortorici et al. (2008) reported that 85% of dental cysts were radicular.
-
Not all lesions that present with a low-density appearance remain low density. A number of entities such as focal osseous dysplasia (Figs. 15.38, 15.39 and 15.40) and ossifying fibroma progress radiographically from low-density to mixed density and finally mature to high-density lesions.
-
Two conditions are associated with multiple, bilateral multilocular low-density lesions. Cherubism (Fig. 15.41) is easily identified presenting with bilateral, almost symmetrical, multilocular radiolucencies (giant cell lesions) affecting the posterior mandibular and commonly maxillary sextants in children, adolescents, or young adults. They generally undergo complete regression to lamella bone (MacDonald 2011). Multiple tumors keratocystic odontogenic tumors (KCOT) appear in approximately 2/3rds of patients with nevoid basal cell carcinoma syndrome (NBCCS) (Fig. 15.42) (MacDonald 2011). These syndromic KCOTs present in the second and third decades, on average a full decade earlier than the solitary (non-syndromic) KCOTs. New lesions continue to form and since they are neoplasms, continue to grow.
-
Not all periapical unilocular low-density lesions should be considered of inflammatory origin. In the anterior maxilla periapical inflammatory lesions (Fig. 15.43) must be distinguished from nasopalatine duct cysts (NPDC) (Fig. 15.44), particularly if they are associated with the central incisors. Although NPDC account for only 1% of all cysts of the jaws, if left untreated they can continue to grow and expand into the nasal cavity, distorting adjacent anatomy (Suter et al. 2011). Although the adjacent teeth are usually vital, these so-called fissural cysts may become secondarily infected (Faitaroni et al. 2011).
-
Basal cell carcinomas present significantly more frequent in NBCCS cases in North Europeans in comparison to East Asians, whereas KCOTs present significantly more frequently in East Asians. PTCH was expressed significantly more frequently in syndromic KCOTs than in non-syndromic KCOTs (MacDonald 2015b). The recurrence rate of syndromic KCOTs was significantly greater than of the solitary KCOTs. The reader should note however that non-syndromic cases with multiple KCOTs could be more common in East Asians (MacDonald et al. 2015).
-
The most common odontogenic cyst is the radicular cyst. This a unilocular, round or ovoid in shape, well-defined, uniform, low-density entity which is identified in the apical region of necrotic tooth and it is considered inflammatory in origin (Fig. 15.45). Most often it is circumscribed by a thin corticated border which may disappear if the osseous boundaries in which it is contained are compromised (Fig. 15.46) or may become thicker with chronic inflammation. It is the second most frequently seen periapical radiolucency after the periapical granuloma from which it is impossible to distinguish radiologically. It is generally accepted that larger lesions (greater than 16 mm in diameter) with the radiologic features described above are most often radicular cysts and smaller, with the same appearance, are most frequently periapical granulomas.

Reformatted panoramic (a) and cross-sectional images (b) of the right posterior mandible depicting a small, well-defined, low-density lesion in the apical region of the second molar. This area of chronic apical periodontitis is most likely a result of pulpal necrosis. Periapical inflammatory lesions are the most common low-density lesions of the jaws

Axial images at the alveolar (a) and basal (b) bone level and a posterior coronal (c) image showing a radicular cyst in the right posterior mandible associated with a carious molar tooth. The entity is unilocular, has expanded and eroded the lingual cortex, showing a fistulas tract in the alveolar crest, buccal to the carious tooth. (Images courtesy of Thomas Li, Elsevier (MacDonald 2016))


Axial (a), posterior coronal (b), and anterior trans-axial (c) CBCT images of the mandible of florid osseous dysplasia in a middle-aged female of East Asian origin. Multiple radiolucencies are present throughout the mandible, the largest of which are present in the premolar-molar alveolus bilaterally, sparing the basal bone. These larger lesions exhibit a multilocularity and thin and erode the cortex with minimal expansion. The anterior lesions appear to arise as ill-defined discrete radiolucencies with small internal calcific foci associated with individual teeth (Images courtesy of Thomas Li, Elsevier (MacDonald 2015a))


Series of cross-sectional images (a) and a reformatted panoramic image (b) of the anterior mandible depicting multiple small, well-defined, low-density lesions in the apical region of anterior teeth with intralesional globular high-density areas. This appearance is consistent with periapical cento-osseous dysplasia (PCOD) of a mature stage. The entities start as low-density entities and gradually obtain high-density centrally located masses as they mature with time

Series of cross-sectional images (a) and a reformatted panoramic image (b) of the right posterior mandible depicting a large, well-defined, low-density entity surrounded by a corticated border associated with the mesial aspect the root of the visible molar. This contains a large high-density globular mass (mature stage). This imaging appearance is consistent with focal osseous dysplasia, a similar entity to POD entity, only in that it is solitary and may appear in any region of the maxilla and mandible and not necessarily limited to the apical region. This entity also undergoes radiographic transformation through different maturity stages

Reformatted panoramic (a), facial 3D surface projection (b) and left lateral 3D surface projection (c) from CBCT data of a teenager with cherubism. The multilocular lesions affect the entire mandible and maxilla. The buccolingual expansion is symmetrical

Reformatted panoramic (a), axial (b), and coronal (c) CBCT images of a patient with Nevoid Basal Cell Carcinoma Syndrome (NBCCS). Note the multiple radiolucencies (KCOT) in the mandible bilaterally and one in the posterior right maxilla. Two of the mandibular lesions are unilocular with corticated margins, whereas one on the right is multilocular and demonstrates substantial thinning but minimal expansion of the lingual cortex. The maxillary lesion obliterates the lumen of the right maxillary sinus. (Images courtesy of Thomas Li, Elsevier (MacDonald et al. 2016)

Axial CBCT images from three individuals—(a, b, and c)—showing radicular cysts occurring in the anterior sextant of the maxilla. Images (a) and (b) show erosion and expansion of the buccal and palatal cortices and intimate but separate relationship to the nasopalatine canal. (Image (a) courtesy of Alexandre Khaireallah; images (b) and (c) courtesy of Thomas Li, Elsevier (MacDonald 2016))

Reformatted panoramic (a) and sagittal (b) image of maxillary edentulous patient with nasopalatine duct cyst. (Figure courtesy of Alexandre Khaireallah, Elsevier (MacDonald 2016))

Reformatted panoramic (a) and serial cross-sectional images (b) of the anterior maxilla depicting a round, well-defined, low-density entity in the apical region of the left lateral incisor with thinning of the palatal cortical plate. Together with the clinical history that this tooth was non-vital, the imaging appearance is most consistent with a radicular cyst

Axial orthogonal image (a), reformatted panoramic image (b), and a series of cross-sectional images (c) of the anterior maxilla depicting a round, moderately defined, low-density entity in the apical region of the left lateral incisor with erosion of both buccal and palatal cortical plates. Despite the fact that this tooth appears to be “floating” due to lack of osseous support, the imaging presentation is most consistent with a radicular cyst
If the tooth involved in the origin of a radicular cyst is extracted and the radicular cyst is not removed, this cystic lesion may remain and continue to grow irrespective of the absence of the tooth that initiated it. While histologically identical to a radicular cyst, it is now referred to as a residual cyst (Fig. 15.47).


Reformatted panoramic (a) and a series of cross-sectional images (b) of the left posterior maxilla depicting a round, well-defined, low-density entity in the premolar edentulous region. The lesion has a thin corticated border and expanded both buccal and palatal cortices. The imaging appearance is suggestive of a residual cyst
The glandular odontogenic cyst (GOC) is another lesion of growing importance, only recently described (Fig. 15.48). This is a rare, slow-growing entity which presents predominantly in the fifth decade most frequently in those of European or Middle-Eastern origin (Macdonald-Jankowski 2010). It can be either unilocular or multilocular in appearance and most are well defined with almost 1/3rd presenting with root resorption. These features may resemble lesions like radicular cysts or unicystic ameloblastomas from which the differentiation of GOC is difficult. Approximately 18% recur (MacDonald 2011).
-
The most common pericoronal radiolucency is the dentigerous cyst (DC). Dentigerous cysts are unilocular radiolucencies which are associated with the cemento-enamel junctions (CEJ) of unerupted and impacted teeth. They are the second most common cyst, after the radicular cyst. They may occasionally be symptomatic if secondarily infected or associated with fracture. They most often present in the second and third decades with a slight predilection for males. Approximately 50% occur in association with the mandibular third molars (Fig. 15.49). Other sites, in decreasing order of frequency, include the maxillary canines (Fig. 15.50), mandibular premolars, and maxillary third molars. They have a low recurrence rate. They present radiographically with all the hallmark features of a cyst including a well-defined, corticated unilocular homogeneous expansile radiolucency with displacement of involved teeth and root resorption of adjacent teeth. If a pericoronal space (normal value up to 3 mm wide) is greater than 3–5 mm, then a DC should be considered. In addition if the attachment of a pericoronal lesion is less than 1 mm apical to the cemento-enamel junction (CEJ), a DC is highly probable. The DC presents in one of the three radiographic patterns: Classical—symmetrical enveloping of the unerupted tooth; Lateral—arising from the side of a crown; and Circumferential—extension of the lesion below the CEJ. Possible sequelae include conversion of the cystic ling to KCOT, unicystic ameloblastoma, and rarely malignant neoplasm (squamous cell carcinoma or mucoepidermoid carcinoma). Dentigerous cysts are often associated with odontomas (MacDonald 2011).
-
The most common neoplasms associated with the alveolus and teeth are odontogenic in origin. The most frequent neoplasm is the ameloblastoma and keratocystic odontogenic tumor (KCOT).
-
Ameloblastoma. The vast majority of ameloblastomas present within the jaw bone and are sub-classified as solid (multilocular) (Fig. 15.51), unicystic (Fig. 15.52), and desmoplastic (Fig. 15.53). Root resorption is a prominent feature, especially “knife-edge” pattern. Root resorption is also associated with other jaw lesions, including KCOT, but with less severity (Fig. 15.54) and frequency (MacDonald 2011). Another feature of AMB is substantial buccolingual expansion (Figs. 15.2 to 15.54), which is more “ball-like” than that of KCOT (Fig. 15.55).
-
Keratocystic Odontogenic tumor. The term keratocystic odontogenic tumor (KCOT) was introduced in 2005 by the 3rd WHO classification to replace the original term keratocystic odontgenic (OKC) to reflect its neoplastic attributes, which included a marked tendency to recur. Interestingly the author of this change was Philipsen, who originally coined the original term of OKC.The 4th edition of 2017 advocated that KCOT be changed back to OKC and that it no longer be considered to be a neoplasm, butrather a developmental cyst (Speight et al. 2017). Unfortunately this reasoning was largely based of out-dated publications. One of these initially indicated that the KCOT responded to marsupialisation, which was used by the WHO authors as evidence of the KCOT being a cyst rather than a neoplasm. Unfortunately, subsequent follow-up of these marsupialised cases revealed recurrences, which led not only to a partial retraction of the initial publications but the lead author (Pogrel) of that early work later showed by systematic review that the current preferred treatment for KCOT, namely enucleation with adjuvant treatment, was more effective that marsupialisation (Al-Moraissi et al. 2016). Therefore, the term KCOT will be retained.
-
-
Non-odontogenic conditions should always be considered in the differential diagnosis of low-density conditions. Generally odontogenic pathological entities may appear in the broader tooth-bearing zone of the maxilla and mandible (alveolar bone) whereas non-odontogenic lesions tend to present in both tooth-bearing and non-tooth-bearing areas of the maxillofacial region. These entities usually originate from the osseous tissues, however other origins should be considered. The diagnostic path for a differential diagnosis is somewhat clearer if these lesions appear in non-tooth-bearing areas (base of the alveolar bone, bony cortices, inside osseous canals, etc.). Developmental anomalies or anatomical variants may add some complexity to the diagnostic process.
-
Lingual bone defect (Stafne’s bone cavity, Stafne’s defect, submandibular gland depression). Appearing as a distinct unilocular radiolucency on panoramic imaging, the lingual bone defect (LBD) shows as a specific well-defined lingual cortical discontinuity (Fig. 15.56). On the panoramic images most LBD present in the basal process of the posterior mandible, in relation to the submandibular fossa, below or substantially below the mandibular canal. The location and corticated border of this entity on reformatted panoramic images raise the level of suspicion while the shape (semispherical concavity) in MPR images or cross-sectional images and location to the mandibular canal should confirm the pathognomonic presentation. On occasion, the LBD presents at the level of the mandibular canal or higher (Fig. 15.57). Although large LBDs may reduce the structural integrity of the mandibular body, pathologic fracture associated with this entity has not been reported. LBDs should be differentiated from aggressive, soft tissue pathological entities originating from the floor of the mouth and may be invading the lingual mandibular cortex (Fig. 15.58). LBD may present anteriorly adjacent the sublingual gland, where differential diagnosis includes simple bone cyst and periapical radiolucencies.
-
Simple bone cyst (traumatic, idiopathic, or hemorrhagic bone cyst). (Fig. 15.59 and 15.60). Despite its name, the simple bone cyst (SBC) is not a true cystic lesion as it lacks an epithelial lining. It is a non-odontogenic condition of unknown etiology also occurring in the axial skeleton. In the maxillofacial region, the SBC occurs frequently in children, teenagers, and young adults with a possible relationship to previous trauma and orthodontic treatment (Velez et al. 2010). Mathew and co-authors (2012) have described the etiology of SBC in detail. The SBC is most frequently seen in the mandible (molar and premolar region) and as an incidental finding on routine panoramic radiographs. The SBC presents as a well-defined low-density cyst-like entity, round or ovoid in shape; it may be associated with the periapical area and extend superiorly between the roots of the teeth to involve the tooth-bearing areas producing a scalloped outline. The teeth involved are vital and show an intact lamina dura. In the jaws it may achieve considerable mesiodistal extension, but with little buccolingual expansion, although large lesions have been reported (Mathew et al. 2012). SBC must be distinguished from other lesions, such as the KCOTs, that require treatment. Commonly definitive diagnosis is only established at surgery when a cavity devoid of an epithelium is found. Recurrence rate is reported to be low in most, but not all reports (Suei et al. 2010) with multiple recurrences especially in middle-aged females (MacDonald-Jankowski 1995). Radiographic features associated with higher recurrence include loss of lamina dura, root resorption, nodular bone expansion, multilocularity and the concomitant presence of osseous dysplasia (Suei et al. 2010). Chadwick and co-authors (2011) report that while solitary SBCs occur equally in either gender in young individuals, those associated with osseous dysplasia occur in older almost exclusively female individuals. The reports of MacDonald-Jankowski would suggest that many of these patients may be of East Asian origin (MacDonald-Jankowski 1995).
-
Brown tumor of hyperparathyroidism. This is a rare cyst-like entity of the bone and represents a giant cell tumor as a result of abnormal calcium turnover in patients with hyperparathyroidism (primary or secondary). Although brown tumors may show in different bones (pelvis, femur, ribs, etc.) they are most common in the jaws; their radiologic appearance is that of a unilocular or multilocular low-density lesion, moderately or poorly defined which may present in any region of the jaws, both tooth- and non-tooth-bearing (Fig. 15.61). A case of a brown tumor was considered to be an ameloblastoma prior to biopsy (MacDonald 2012).
-

Intraoral periapical (a), cropped reformatted panoramic (b), axial (c), and trans-axial (d) CBCT images of a glandular odontogenic cyst arising in the premolar-first molar area of the mandible. The lesion shows as a relatively ill-defined unilocular radiolucency, resorbing the apical half of the second premolar. There is some buccolingual expansion, extension from the alveolus into the basal process and erosion of the superior cortex posteriorly. The mandibular canal is displaced inferiorly (Images courtesy of Elsevier (MacDonald 2016))

Axial (a) and coronal (b) image of CBCT data showing a dentigerous cyst arising from the CEJ of an unerupted right mandibular molar. Note the bilateral mandibular tori arising adjacent to the pre molars (Images courtesy of Thomas Li)

Reformatted panoramic (a) and serial trans-axial images (b) of CBCT data showing a dentigerous cyst arising from a left unerupted maxillary canine. Note buccolingual expansion, and perforation of the labial (buccal) and palatal cortical plates (Figure courtesy of Wiley-Blackwell), (MacDonald 2011)

Axial section of CBCT data showing an ameloblastoma (histopathologically solid type) in the anterior mandible. A single internal septa transects the lumen horizontally making this a multilocular lesion. The lesion demonstrates substantial displacement and erosion of the buccal cortex and some displacement and erosion of the lingual cortex. (Image courtesy of Jason Chen and Elsevier MacDonald D (2016))

Axial (a) and coronal (b) images of a unicystic ameloblastoma associated with an unerupted and impacted right mandibular third molar in a Chinese patient from Hong Kong. The lesion has significantly expanded and eroded the lingual cortex of the mandible to create an almost circular outline. The expanded lingual cortex has been displaced downward and past the lower border of the mandible, a feature previously reported on conventional images of this neoplasm (MacDonald 2011). Note that the buccal cortex is eroded at a single focus and the root of the second molar exhibits significant resorption. (Images courtesy of Thomas Li, Elsevier (MacDonald 2016))

Axial (a), cropped coronal (b), and trans-axial (c) CBCT images of a desmoplastic ameloblastoma in the right anterior maxilla. This neoplasm presents with an irregular, substantially corticated margin. Some broad-based septae are present and therefore the lesion is multilocular. It spares the anterior recess of the right maxillary sinus. Benign aggressive features include erosion of the palatal cortex of the alveolus, resorption of the distal aspect of the apical half of the root of the canine with irregular surface erosion on the palatal aspect of the cervical half of the root. (Image courtesy of Kenneth Chow, Elsevier (MacDonald 2016))

Thin section reformatted panoramic (a), axial (b), and serial trans-axial (c) images of a keratocystic odontgenic tumor (KCOT) arising in the anterior maxilla. The lesion extends from the midline to the junction between the second premolar and first molar area with apparent occlusion of the superior half of the nasopalatine canal. The lesion has displaced and eroded the anterior wall and adjacent floor into the lumen of the left maxillary sinus. The buccolingual dimension is about half of that of its mesiodistal extent. Furthermore, although essentially unilocular, the expansion is variable. An unerupted tooth is observed within the neoplasm. (Images courtesy of Jason Chen, Elsevier (MacDonald 2016))

Reformatted panoramic (a) and series of cross-sectional images (b) of the right posterior mandible depicting a multilocular, well-defined, low-density entity in the apical region of the premolar and molar teeth. The lesion has a thin corticated border and although expanded both buccal and palatal cortices. The imaging appearance is suggestive of KCOT in the region of the first molar

Comparative panoramic images from 2010 (a) and 2013 (b) and 2013 parasagittal (c) axial (d) and trans-axial (e) CBCT images of a lingual bone defect LBD) appearing as a well-defined unilocular radiolucency in the right mandible. Minor extension of the entity is noted in the 2013 panoramic image associated with the removal of the third molar. CBCT images show upward displacement of the mandibular canal with a loss of its inferior cortex seen as a dehiscence of the canal in trans-axial sections. (Images courtesy of Lief Kullman, Elsevier (MacDonald 2016))

Reformatted panoramic (a) and a series of cross-sectional images (b) of the right posterior mandible showing a deep lingual concavity which was diagnosed as a lingual bone defect (LBD). Diagnostic confusion may exist due to the fact that the entity is at the level of and appears to involve the left mandibular canal (red arrows)

Reformatted panoramic (a) and series of cross-sectional images (b) of the left posterior mandible depicting a lingual concavity occupying the lower half of the mandible in the molar region and appearing to involve the mandibular canal. The irregular internal border of this entity increases the level of suspicion towards an invasive soft tissue mass from the floor of the mouth. Clinical correlation and comparison to previous radiographic examinations confirmed this to be a lingual bone defect

Reformatted panoramic (a) axial (b) and cross-sectional image (c) in the region of the left anterior mandible showing a fairly well-defined, low-density, cystic entity which has caused uniform thinning and expansion of the lingual and labial cortex (orange arrows). Also note that the lesion is scalloping between the roots of involved incisor and canine teeth. The above features are suggestive of a SBC

Reformatted panoramic (a), axial (b), and single cross-sectional image (c) of the mandibular anterior region showing fairly well-defined, low-density, cystic entity inferior to the right canine which has resulted in thinning and expansion of the labial cortex (orange arrows). The lesion is clearly in a non-tooth-bearing area and its appearance consistent with a diagnosis of a SBC

Reformatted panoramic (a), axial (b), and a series of cross-sectional images (c) of the right mandible showing multiple, moderately well-defined, low-density entities, throughout the mandibular bone. Some of the lesions imitate periapical pathologies (red arrows), however there generalized presentation suggest a systemic or developmental condition. Based on the clinical presentation and medical history, a working diagnosis of giant cell tumors of primary hyperparathyroidism was established and subsequently confirmed
3.2 High-Density Lesions
Hyper-attenuating entities most often have well-defined borders that are associated with benign lesions representing slow-growing excessive formation of normal bone (e.g., exostoses and osteoma) or replacement of bone with odontogenic (e.g., odontoma, cementoblastoma) fibro-osseous (e.g., fibro-osseous lesions) or bone (e.g., enostosis, dense bone islands, osteoblastoma).
-
Odontomas are the most common benign odontogenic tumors of the jaws. Odontomas present as an asymptomatic well-defined heterogeneous hyper-attenuating expansive mass, limited to the alveolus, with a radiolucent rim often associated with the failure of eruption of a permanent tooth. Most occur in the maxilla. Radiographically odontomas present in one of two patterns:
-
Compound. Multiple small tooth-like structures, not greater than the diameter of the associated tooth (Fig. 15.62).
-
Complex. A single radiopaque mass, tending to be round or ovoid with a round or smooth margin having density greater than bone (Fig. 15.63).
Presentation and location depends on type of radiographic pattern. Compound odontomas more frequently occur in the anterior maxilla in teenagers whereas complex odontomas arise commonly in the posterior regions in young adults. If untreated, a high proportion develop into cysts (cystic odontoma) which may become secondarily infected (Fig. 15.64).
-
-
Exostoses are the most common benign non-odontogenic tumor of the jaws. Exophytic smooth surfaced self-limiting benign tumors of bone result in localized cortical exostosis which arise most often at three specific locations:
-
Mandibular Torus (MT). MT are bilateral smooth surface well-defined exostoses arising from lingual alveolus of the mandible above the mylohyoid ridge in the region of the premolars (Fig. 15.65). Size may vary from small raised cortical bumps to large extensive pedunculated multi-nodular masses (Figs. 15.49 and 15.65). Rare in children and teenagers, MT is usually established by the fourth decade with a male predominance. It is a common with a variable incidence depending on ethnic group (range, 2–25%). Predominantly has a hereditary etiology (autosomal dominant) with contributing environmental factors such as occlusal stress associated with parafunctional habits and long-term use of phenytoin. MT is associated with other regional exophytic growths including buccal exostoses (up to 36%) and torus palatinus (up to 50%) which can be identified by clinical intraoral examination.
-
Torus palatinus (TP).TP is a midline hard palate exostosis, more frequent than MT and more common in women. Typical radiographic patterns can be uni- or multi-lobulated, flat and spindle-shaped (Fig. 15.66).
-
Alveolar exostosis. Alveolar exostoses can arise on the alveolus adjacent the cervical third of the roots of posterior teeth on either the palatal/lingual or, more commonly, the buccal aspect. Exostoses are more common in the maxilla than in the mandible (5.1:1) and prevalence increases with age. Exostoses are more common in men than in women and appear concurrently with MT than with TP (Fig. 15.67).
They present as asymptomatic exophytic masses that may increase in size slowly over time. Larger lesions may become nodular and can be multiple. They may appear as a uniformly homogeneously hyperdense expansion of the cortical plate (compact bone variant) or as an extension with an outer cortical plate and inner medullary bone (cancellous variant). Tightly bound thin mucosa may become traumatized.
-
-
Incidental high-density benign intramedullary entities are common. These include:
-
Idiopathic osteosclerosis (dense bone island). Idiopathic osteosclerosis (IO) is a benign entity characterized by uniformly dense bone (similar to that of cortical bone) which extends with variable shape and size within the intramedullary area between the cortical plates of the alveolus. While IO is often restricted in the alveolar bone, it may spread to the base of the maxillary or mandibular bone. IO is more frequently seen in mandible and of unknown etiology (MacDonald-Jankowski 1999). IO may cause root displacement and sometimes even root resorption. IO should be differentiated from condensing osteitis and various forms of osseous dysplasia (OD) including mature periapical, focal, and florid osseous dysplasia. IO can occasionally present with radiographic features similar to osseous dysplasia or ossifying fibroma (OF) on conventional radiography. This may arise from the difficulty in discerning the “Mach band effect” (MacDonald 2011) adjacent to a central hyperdense lesion from a radiolucent border around OFs and most ODs (Figs. 15.68 and 15.69). A characteristic CBCT imaging feature is the presence of trabeculae extending from the periphery.
-
Condensing osteitis. Condensing osteitis (CO) is characterized by the presence of sclerotic (dense) bone resulting from a local inflammatory response (McDonnell 1993), most commonly periapical in origin. The radiographic appearance of CO is similar to IO; however, CO is associated with mostly non-vital teeth with concomitant widening of the periodontal ligament space (Fig. 15.70)
-
Osteomas. Osteomas are benign osseous masses that consist solely of cortical bone or a periphery of cortical bone and a central cancellous bone core. The most common are peripheral, and project from a bony surface, or they may be central, originating from the endosteum and projecting into the cancellous bone. They are uncommon and may also present in the frontal and ethmoid sinuses, maxillary sinuses, and in the mandible. Peripheral osteomas are readily identified because of their exophytic nature, whereas central osteomas appear similar to IO, CO, and odontomas (Kaplan et al. 2008) (Fig. 15.71).
-

Axial (a), parasagittal (b), and coronal images (c) of the right posterior maxilla showing an irregular, high-density mass that looks like a malformed tooth (contains both enamel and dentin elements) surrounded by a large cystic entity. Imaging appearance is similar to a resorbing third molar except for the irregularity of the enamel portion centrally. This imaging appearance is most consistent with a compound cystic odontoma

Axial (a), cross-sectional (b), and parasagittal (c) images of the left anterior maxilla in the region of the premolar and canine showing multiple high-density, tooth-like structures surrounded by a wide low-density zone and a corticated border that resembles a tooth follicle. The lesion is slightly expansile and has thinned the buccal cortex. The imaging appearance is pathognomonic with a compound odontoma

Panoramic (a) and subsequent axial (b) and series of cross-sectional CBCT images (c) showing an amorphous globular high-density mass in the left posterior maxilla associated with the pericoronal aspect of a first molar. The mass is surrounded by a wide low-density zone and a corticated border with some expansion on the buccal and palatal cortices. The mass demonstrates varying densities, some of which correspond with the density of enamel. The imaging features are pathognomonic for a complex odontoma

Axial (a) and coronal (b) images showing large pedunculated osseous masses on the lingual aspect of the mandibular bone adjacent to the premolars, radiographically pathognomic for bilateral mandibular tori

Axial (a), coronal (b), and midsagittal (c) images of the maxillary palatal region showing a large pedunculated osseous mass along the midline of the hard palate, radiographically pathognomic for torus palatinus

Axial (a) and coronal (b) images showing large pedunculated bilateral osseous masses on the palatal aspect of the maxillary alveolus consistent with a diagnosis of buccal maxillary exostoses. Note also the torus palatinus in the coronal image

Reformatted panoramic (a) and series of cross-sectional images (b) showing a large, irregularly shaped, homogenous, high-density lesion involving the roots of the right second molar extending below the alveolus. The imaging appearance is consistent with idiopathic osteosclerosis

Reformatted panoramic (a) and a series of cross-sectional images (b) of the mandibular left posterior region showing a localized elongated hyperdense area resorbing the mesial root of the first molar (arrows). The imaging appearance is consistent with idiopathic osteosclerosis

Reformatted panoramic (a) and a series of cross-sectional images (b) of the mandible showing a large, diffuse, mostly homogenous high-density lesion, associated with the apices of the left first molar and pericircumferential alveolar bone loss associated with both roots. This is consistent with reactive sclerosis induced by chronic inflammation from this tooth. The imaging appearance is consistent with condensing osteitis

Reformatted panoramic (a) and a series of cross-sectional images (b) of the mandible showing an exophytic, round, homogenous, high-density pedunculated mass extending from the lower border of the right mandible consistent with a radiologic diagnosis of osteoma
3.3 Mixed Density Lesions
Apart from the homogenous low-density and high-density entities addressed in earlier, there is a number of entities that demonstrate a mixed appearance; these may include cyst-like lesions (mostly low-density radiolucent) which contain high-density foci or lesions that demonstrate a mixture of different densities throughout the lumen of the lesion. The varying density levels may represent different degrees of mineralization for several of these entities; in fact, as some of these entities mature, they change in appearance from an initial low density to a mixed density and finally to high density as their content becomes gradually more mineralized. Some of these lesions are associated with teeth and others are not.
3.3.1 Tooth-Related Mixed Density Pathological Entities
Mixed density entities mat present in association with the crown of an impacted or unerupted tooth (pericoronal) or in the periapical region of the maxillary or mandibular teeth. Pericoronal entities that present as mixed density lesions are rare; however, many have characteristic demographics or imaging characteristics that help in diagnosis (Table 15.8).
Unlike their pericoronal counterparts, periapical mixed density lesions are relatively common.
-
Periapical osseous dysplasia (POD). The intermediate stage of POD presents as a mixed density periapical lesion which progresses to a high-density lesion when it is completely matured. Radiographic variation in presentation is related to the three stages in the maturation of the lesion. POD is considered a localized form of osseous dysplasia and while the etiology is unknown, it is thought to be linked to elements within the periodontal ligament. Initially POD presents as a well-defined, low-density periapical area, sometimes surrounded by a corticated border. At this stage no expansion is observed. It is more common in the mandible affecting the anterior sextant only (Figs. 15.72, 15.73, 15.74, and 15.81). At the intermediate/mature stage, POD lesions contain high-density internal globular masses which may range in number and vary in form from tooth to tooth if multiple teeth are affected. The involved teeth are vital, however concurrent chronic apical periodontitis may occur minimal. At this stage POD may cause thinning or minimal expansion of the cortical plates locally and may affect more than one tooth. Any appreciable expansion of an OD should prompt consideration of expansive OD (Noffke et al. (2012). POD requires no treatment but periodic intraoral radiographic assessment to monitor transition is suggested.
-
Cementoblastomas. Cementoblastomas are rare, benign odontogenic tumors which originate from the cementum of the root of a tooth; they appear as a well-defined and regularly shaped exophytic homogeneous mass of cementum or cementum-like tissues apparently fused to the root. They have a mixed or high-density presentation and may be surrounded by a thin hypodense peripheral rim. They are often round or ovoid in shape and may cause expansion of the jaw in the region they develop. They most frequently present associated with the roots of the mandibular premolars and molars (Figs. 15.75).

Reformatted panoramic (a) and a series of cross-sectional images (b) of the mandible depicting a well-defined, mixed density lesion associated with the apex of the right premolar containing up to two discrete globular masses with a low-density uniform periphery. The lesion has expanded and thinned the lingual mandibular cortex. The radiologic findings are consistent with periapical osseous dysplasia

Reformatted panoramic (a) and a series of cross-sectional images (b) of the mandible depicting multiple well-defined, mixed density lesions associated with the incisor teeth demonstrating central globular masses. Similar to the patient in Fig. 15.72, the lesions have expanded and thinned the lingual and labial mandibular cortex. The radiologic findings are consistent with periapical osseous dysplasia

Reformatted panoramic (a) and a series of cross-sectional images (b) of the anterior maxilla) depicting a single, well-defined, mixed density lesion associated with the root of the right canine demonstrating up to four central globular masses with a peripheral hypodense zone. The lesion has expanded and thinned the labial and palatal maxillary cortex. The radiologic findings are consistent with early expansive osseous dysplasia

Reformatted panoramic (a), axial (b), and parasagittal (c) image of the maxilla and mandible showing a large, round inhomogeneous spiculated globular mass associated with the roots of the right mandibular second molar surrounded by thin uniform hypodense rim. Although the radiologic findings are consistent with a benign cementoblastoma, the lack of root resorption and fusion with the root also prompt consideration of ossifying fibroma
3.3.2 Mixed Density Jaw Pathology, Not Associated with Teeth
-
Fibro-osseous lesions (FOL). FOL represent an important group of mixed or high-density lesions affecting the jaws. FOLs include fibrous dysplasia, ossifying fibroma, and osseous dysplasia. Until recently, large FOLs were most often imaged by MDCT. Smaller FOLs are often asymptomatic and discovered as an incidental finding on conventional dental radiography. With increasing availability of CBCT units in general and specialist dental offices, the radiographic features of FOLs are now being characterized on CBCT images. Regarding FOLs, the late Charles Waldron, state that:
In absence of good clinical and radiological information a pathologist can only state that a given biopsy is consistent with a FOL. With adequate clinical and radiological information most lesions can be assigned with reasonable certainty into one of several categories.
Conversely, in the absence of such information, Eisenberg and Eisenbud stated (MacDonald-Jankowski 2004; MacDonald 2011):
…pathologists today will often rightly decline to render a definitive diagnosis…. Instead, the pathologist will resort to the noncommittal designation of benign fibro-osseous lesions (their italics). This is the only acceptable approach considering the potential for inappropriate treatment otherwise.
-
Fibrous Dysplasia (FD). FD is a slow-growing, usually self-limiting, benign fibro-osseous disease in which normal bone and marrow are replaced by fibrous tissue and irregularly distributed woven bone (Figs. 15.76 and 15.77). The most common locations are the craniofacial bones, proximal femur, and rib. Gnathic FD is referred to as a fibro-osseous lesion. Approximately 80% of individuals present with FD affecting one bone (monostotic) with the remaining affecting multiple bones (polyostotic) either with (McCune-Albright syndrome) or without endocrinopathies.
Polyostotic FD involving contiguous bones in the skull, such as the maxilla and zygoma, is referred to as craniofacial FD (Fig. 15.78). This disease is found in the third decade with a male predilection, especially in younger individuals (MacDonald-Jankowski 2009). Progression tapers with skeletal maturity however does not regress to lamellar bone and persists throughout life (MacDonald 2011). Most lesions become quiescent; however, the reactivation rate is approximately 18%.
Most commonly individuals present with painless, slow-growing asymptomatic facial swelling (MacDonald-Jankowski 2009) associated with uniform buccolingual expansion. Management is dependent on anatomic site, degree of involvement, patient’s age and stage of skeletal maturity and anticipated growth potential. Surgery is only indicated for esthetic reasons, impaired function (e.g., opening or tooth occlusion), pain due to constriction of neurovascular foraminae, or optic nerve encasement.
FD has poorly defined margins which distinguishes it from OF which has well-defined margins. This distinction is most clearly observed in the mandible and in the alveolus of the maxilla. Although not strictly necessary for a diagnosis of FD, a biopsy is necessary to confirm the diagnosis of OF since this lesion needs to be completely removed or resected, depending on size (MacDonald 2011).
-
Ossifying Fibroma (OF). OF is a rare benign slow-growing neoplastic fibro-osseous lesion of the jaws, occasionally involving the mid-facial bones and paranasal sinuses (Figs. 15.79 and 15.80). It usually presents as an asymptomatic, unilateral hard facial swelling, often in the mandible. Maxillary sites often result in extensive sinus involvement. OF has a female predilection with the highest incidence of presentation in the second to fourth decades. The more aggressive, rapidly growing variant with intralesional psammomatous or trabecular calcifications and lack of radiographic capsule may occur in younger individuals (Juvenile OF). Presentation may be syndromic, associated with familial hyperparathyroidism or synchronous with other conditions such as aneurysmal bone cyst. Histopathologically presents as an encapsulated neoplasm of varying quantities of bone, osteoid and cementum-like material in a fibrous connective tissue stroma. Recurrence rate is moderately high (up to 12%). Treatment involves surgical curettage or resection ± reconstruction.
Like other fibro-osseous lesions, OF has three radiographic patterns. OF presents initially and most commonly as a small to moderately sized, round to ovoid smooth expansile hypodensity with well-defined, egg-shell like sclerotic borders. Buccolingual expansion is symmetrical. The entity changes to mixed lesion with more prominent internal centrally located hyperdensity with increasing size ranging from fine, evenly distributed “snow flakes” to a fine, coarse or dense reticular pattern with or without globular dense opacities. Characteristic hypodense peripheral rimming occurs adjacent to the peripheral margin. Lesions can occur inter-radicularly, displacing teeth but not associated with root resorption. In the mandible, the inferior alveolar canal is displaced inferiorly. There is no perforation or associated periosteal reaction.
-
Osseous Dysplasia (OD). Two well-recognized variants of OD exist with radiographic presentations so distinctive that biopsies are rarely required. Histopathology confirmation of an OD lesion only becomes available when an infected lesion needs to be surgically removed (MacDonald 2011).
-
Florid Osseous Dysplasia (FOD). The multiple sextant involvement of OD is a well-recognized radiological phenomenon particularly among middle-to-old aged females of sub-Saharan African or East Asian (Fig. 15.81).
-
Focal Osseous Dysplasia (FocOD).Another form of OD, which may be multiple, but localized to a single sextant is especially distinctive if confined to the lower anterior sextant (Figs. 15.82, 15.83 and 15.84) (previously periapical cemental dysplasia).
The differential diagnosis of FOLs is challenging. The radiological challenge in the diagnosis of FOLs is greatest when attempting to distinguish between OF and FocOD, particularly when the lesion is small (Fig. 15.85). Although OFs are associated with root resorption, this is not a consistent feature, especially in small lesions. This may present the clinician with a diagnostic dilemma in that a OD misdiagnosed as a FocOD may require surgery latter. The following may assist the clinician is differentiating between FOLs.
-
CBCT provides valuable information in distinguishing OD from OF and FD. Specifically, CBCT imaging identifies the position of the lesion within the alveolar bone and its effect on the cortex. Both OF and OD can cause erosion and displacement of the cortex. Although this is usually minimal, exceptions can arise. OF can be distinguished from the other entities by tooth displacement and root resorption only when the lesion has achieved considerable size. OD rarely increases to such large dimensions (MacDonald 2011). Such lesions when affecting one or more sextants in young individuals of either gender or any ethnic origin (MacDonald 2011) have been called gigantiform cementomas. The term familial is added to these if there is a familial history. The more appropriate term, expansive osseous dysplasia, has been proposed by Noffke et al. (2012).
-
A major feature of OD is that it is most frequently confined to the alveolus, above the mandibular canal in the mandible or below the image of the hard palate in the maxilla (MacDonald-Jankowski 2009). Occasionally, the OD may appear below the mandibular canal (Fig. 15.85) and even unassociated with a tooth (Fig. 15.86). Although the absence of a buccolingual expansion and a well-defined periphery with a radiolucent rim is diagnostic of OD, the diagnosis can only be confirmed at follow-up if there is no increase in size, tooth displacement, or root resorption. Asymptomatic OD in edentulous sites should be left alone unless they occur in a site required for an implant. Then they should be first removed by lateral trepanation to preserve the alveolar ridge and the surgical defect allowed to heal (MacDonald 2011).
-
There is a lack of information on the long-term progression of FD. There are few long-term follow-up studies of FD. The largest study in a Hong Kong Chinese population (MacDonald-Jankowski and Li 2009) reports reactivation of FD in 3 out of 17 cases, with two presenting after 10 years. Therefore, FD, once detected, should have long-term, perhaps life-long follow-up as they may be reactivated by a life event such as pregnancy. While panoramic radiography may be adequate for most cases of FD affecting the mandible, in the maxilla CBCT is likely the modality of choice when clinically indicated (MacDonald 2011).
-
While sarcomatous transformation in FD can be induced by radiation therapy, it is rare in the jaws (MacDonald-Jankowski and Li 2009; MacDonald-Jankowski 2009). However, it may occur in up to 1% of cases of FD affecting the face and skull (Cheng et al. 2012; Ruggieri et al. 1994).
-
-
-
Other entities may appear radiographically similar to FOL. The differential diagnosis of FOL includes idiopathic osteosclerosis (Fig. 15.87) and medication-related osteonecrosis of the jaw (MRONJ).
-
Medication-related osteonecrosis of the jaw (MRONJ). This condition presents radiographic similarities to OD and OF, from which it needs to be distinguished (Fig. 15.88). This is usually achieved with a positive history of bisphosphonate therapy for previous bone cancer (bone metastasis and multiple myeloma) or other diseases such as osteoporosis (Kühl et al. 2012; Treister et al. 2010). Although any lesion that becomes exposed to the oral environment can become infected, suspicion of MRONJ must be entertained of clinical exposed bone for longer than 8 weeks, an accompanying history of bisphosphonate and no prior radiation therapy (Treister et al. 2010). CBCT is superior to panoramic radiography (Treister et al. 2010).
-

Reformatted panoramic (a), axial (b), and coronal (c) CBCT images showing fibrous dysplasia in the left retromolar area involving the trigone and ramus with characteristic poorly defined margins. There is a little buccolingual expansion and the dysplastic bone has a ground glass appearance. (Images courtesy of Dr David Gane, Elsevier (MacDonald 2015))

Reformatted panoramic (a) and coronal (b) CBCT images of monostotic fibrous dysplasia in the right maxillary sinus in an asymptomatic 60-year-old female. The lesion shows an ill-defined ground glass lesion in the right posterior maxilla enveloping the apices of subjacent teeth with superior displacement of the floor of the maxillary sinus, obliterating the lateral aspect of the sinus. The infra-orbital canal is involved. (Images courtesy of Dr Allan Abuabara, Elsevier (MacDonald 2015))

Reformatted panoramic (a), axial image of the mandible (b), coronal image of the sphenoid bone (c), and midsagittal CBCT image (d) showing polyostotic high-density ill-defined ground glass expansion of multiple bones and invasion of the sphenoid and right maxillary sinus. The imaging appearance is radiologically pathognomonic for craniofacial fibrous dysplasia

Reformatted panoramic (a) and trans-axial (b) CBCT images of an OD associated with the apex of the left unerupted and impacted third molar. The lesion presents as a central opacity within a radiolucent periphery inferior to the mandibular canal. There is minimal buccolingual expansion, but considerable erosion of both buccal and lingual cortices

Conventional panoramic (a) and axial (b), and coronal (c) MDCT images of the right mandible showing a well-defined high-density spherical expansion of the right posterior body, associated edentulous alveolus and angle of the mandible. There is smooth expansion and egg-shell like thinning of both buccal and lingual cortices concentrically. Internally there are two regions of hyperdensity, separated from the peripheral cortical bone by a thin hypodense rim. The inferior alveolar canal is intact and displaced inferiorly within the entity. The imaging appearance is consistent with ossifying fibroma (Images courtesy of George Kushner)

Periapical (a) and axial (b) CBCT images of the right mandibular region showing a well-defined ground glass high-density egg-shaped lesion displacing the adjacent premolar teeth. Both buccal and lingual cortices are eroded and there is buccal expansion. The lesion is separated from the normal adjacent bone by a thin radiolucent space. The imaging appearance is consistent with ossifying fibroma. (Images courtesy of Kenneth Chow, Elsevier (MacDonald 2015))

Axial (a) and coronal (b) CBCT images of a patient with medication-related osteonecrosis of the jaws (MRONJ). The right para-symphyseal region of the mandible side shows expansion and sclerosis of the bone adjacent to the sequestrum. The “expansion” represents a periosteal reaction with the creation of ‘new bone’ or involucrum. Note: the two circular small hyperdensities in the midline of the coronal image (b) are the genial tubercles

Reformatted panoramic (a), maxillary (b), and mandibular axial (c) images and coronal image (d) showing generalized globular masses in the alveolus of both jaws. The imaging appearance is radiologically pathognomonic for florid osseous dysplasia

Conventional panoramic (a), reconstructed panoramic (b), axial (c), and serial trans-axial (d) images of florid osseous dysplasia in the left mandible of 60-year-old Chinese woman. There are multiple well-defined globular hyperdensities bilaterally within the alveolus of the mandible (a). On the right mandible the globular hyperdensities are all above the mandibular canal and do not demonstrate buccolingual expansion. All lesions are separated from their adjacent normal bone by a radiolucent rim and variable cortication. (Images courtesy of Raman Sumanth, Elsevier (MacDonald 2015))

Axial (a), coronal (b), and cross-sectional (c) CBCT images of multiple periapical osseous dysplastic lesions in the anterior mandible in a female. The lesions comprise small diameter central hyperdensities within hypodensities. There is little buccolingual expansion. (Images courtesy of Michael Matwychuk, Elsevier (MacDonald 2015))

Conventional panoramic (a) and parasagittal (b), axial (c), and trans-axial (d) CBCT images of focal osseous dysplasia associated with the right mandibular second premolar and the mesial root of the first molar. The lesion comprises a central hyperdensity separated from normal adjacent bone by a hypodense periphery. There is no buccolingual expansion or root resorption however there is effacement of the internal margin of the buccal and lingual cortices. (Images courtesy of Jason Chen, Elsevier (MacDonald 2015))

Conventional panoramic (a) and periapical (b) images of a large dense bone island (also called idiopathic osteosclerosis) associated with a second molar inthe right mandible. Initially the lesions was considered to have a radiolucent rim (a) representing a follicular space. Axial (c), parasagittal (d), and cross-sectional (e) CBCT imaging was performed only after a incisional biopsy reported a histopathologic diagnosis of “cortical bone.” CBCT clearly demonstrates the continuity of the lesion and normal trabeculae throughout

Reformatted panoramic (a) and serial trans-axial CBCT images (b) of an osseous dysplastic lesion within the right ramus of the mandible below the mandibular canal. The lesion comprises a central hyperdensity within a hypodense periphery. Although the lesion is nearly 2 cm in diameter, it is associated with minimal buccolingual expansion
3.4 Periosteal Reaction
Periosteal reaction refers to the reactive bone formation underneath the periosteum as a result of any kind of stimulus. Bone formation under the periosteum may demonstrate certain patterns based on the type of induction stimulus. The pattern of new bone formation in the cortical bone observed on CBCT images may be able to suggest whether the underlying process is of a benign or an aggressive nature. These different patterns of bone formation are based mainly on how fast the stimulating abnormal process progresses; thus the detected radiologic differences broadly called periosteal reaction are a reflection of the speed at which new bone is formed (Fig. 15.89) (Rana et al. 2009).

Diagrammatic representation of patterns of periosteal include solid periosteal (a), multi-layer or “onion skin” (b), thick irregular (c), spiculated “hair on end” (d), and “sunburst” (e) as well as the “Codman’s triangle” (f) (Adapted from Rana et al. 2009)
The speed of new bone formation and thus the detected periosteal reaction is a determinant of the aggressiveness of the stimulating pathological entity and this is why it is important to the diagnostician.
-
Solid. A solid periosteal reaction is associated with benign, non-aggressive, slow-growing conditions like osteoid osteoma and healing osteomyelitis. Radiologically this appears as thin or thick layers of bone (Fig. 15.90).
-
Multi-layer. A faster more aggressive entity may induce a laminated or “onion skin” pattern of periosteal reaction; in this cases multiple layers of bone are noted and this is considered an “interrupted” pattern (Figs. 15.91, 15.92, and 15.93).
-
Spiculated. This pattern of periosteal reaction characterizes very aggressive and fast developing entities, like sarcomas. In this pattern, thin osseous fibers may appear to be spreading out of the bony surface. Spicules may originate either perpendicular to the bone (“hair on end”) or may diverge (“sunburst”) (Figs. 15.94 and 15.95).
-
Codman’s triangle. This pattern is associated with rapidly advancing pathological and results in an elevation of the periosteum at a sharp angle at the periphery of the lesion. This may also be seen in sarcoma.

Axial (a) and cross-sectional (b) CBCT images of a limited FOV scan of the left mandible depicting a “solid type” of periosteal (green arrows). Note the central hypodense region surrounded by a thick hyperdense border. The imaging appearance is suggestive of a long-term local inflammatory reaction, possibly related to the previous apical pathology on the adjacent, now root canal filled, tooth

A series of cross-sectional images of the right posterior mandible illustrating “multi-layer” bone deposition on the buccal aspect of the mandible (red arrows). This type of periosteal reaction characterizes a more aggressive pathological entity than that of the solid type as in Fig. 15.90. Considering the clinical presentation and access to previous radiography, the imaging features are consistent with the diagnosis of Garre’s osteomyelitis

A series of cross-sectional images of the left anterior mandible illustrating “multi-layer” periosteal reaction on the lingual aspect of the mandible (red arrows). Bone deposition is interrupted at specific locations suggesting a rapid and disorganized growth. Considering the clinical presentation and medical history, the imaging features are consistent with the diagnosis of medication-related osteonecrosis of the jaws (MRONJ)


Reformatted panoramic (a) and a series of cross-sectional images (b) of the right posterior mandible showing interrupted “multi-layer” periosteal reaction on the buccal/inferior cortex combined with extensive destruction of the mandibular bone. This appearance is suggestive of a high level of aggressiveness. Considering the clinical presentation and medical history, the imaging features are consistent with the diagnosis of osteomyelitis

Thin slice reformatted panoramic (a) and a series of cross-sectional images of the anterior mandible (b) showing a large, irregular, poorly defined, destructive lesion (yellow arrows). Note the moth-eaten appearance of the mandibular cortex as well as the fine spicules originating from the cortical plate (red arrows). This appearance and periosteal reaction are consistent with a very aggressive entity. Considering the clinical presentation and medical history and biopsy, the imaging features are consistent with the diagnosis of Langerhans cell histiocytosis

Axial section (soft tissue window—left; bone window—right) (a) and MIP reconstruction (b) of the right posterior mandible illustrating a “sunburst” type of periosteal reaction, suggestive of the highest level of lesion aggression. Considering the clinical presentation, medical history and biopsy, the imaging features confirmed the histopathologic diagnosis of osteogenic sarcoma
3.5 The Diagnostic Challenge of the Aggressive Lesion
The most important concern of the clinician in radiologic analysis of CBCT images is to ensure that no serious pathological condition within the volume is missed. Therefore, the distinction between a malignant and a benign lesion is of utmost priority.
Albeit the key imaging features of malignant lesions were characterized previously, it should be noted there is considerable overlap in presentation between benign and malignant conditions that may be difficult to distinguish. These pathological entities include:
-
Osteoradionecrosis
-
Medication related osteonecrosis of the jaw (MRONJ) (Fig. 15.98)
-
Malignant lesions (primary or metastatic) (Figs. 15.99 and 15.100)

Reformatted panoramic (a) and series of cross-sectional images (b) illustrating a massive, poorly defined, mixed lesion occupying the entire right mandibular ramus; note the “moth-eaten” appearance and extensive destruction. This was proven to be osteomyelitis, although a malignant lesion could be considered, based on imaging findings alone

Reformatted panoramic (a) and a series of cross-sectional images (b) illustrating a massive, poorly defined, mixed lesion occupying the entire anterior mandible. Note the erosion of the inferior cortex and extensive destruction of the mandibular bone. Based on clinical presentation, the imaging features suggest osteomyelitis, which was confirmed by biopsy


Reformatted panoramic (a) and a series of cross-sectional images (b) illustrating a large, poorly defined, mixed density lesion in the mandibular right canine/premolar region. Note the localized destruction of the mandibular bone and the diffuse sclerosis extending throughout the mandible. Based on clinical presentation and medical history, the imaging features suggest medication-related osteonecrosis of the jaws (MRONJ), which was confirmed by biopsy


Reformatted panoramic (a) and a series of cross-sectional images (b) illustrating a large, poorly defined, mixed density lesion in the mandibular left premolar/molar region. The entity appears to be surrounded by a wide irregular low-density zone whereas there are signs of considerable destruction of the osseous tissue in the affected area. Inferior alveolar nerve paresthesia was reported. Although similar to the imaging findings presented in Figs. 15.96, 15.97, and 15.98, based on biopsy the final diagnosis was s metastatic carcinoma from the lung

Sagittal (a) sections of the anterior mandible illustrating the “moth-eaten” appearance of the mandibular bone for a patient diagnosed with medication-related osteonecrosis of the jaws. Coronal (b) images of a different patient in the same area demonstrating almost identical radiologic findings. However in the latter case, histopathologic diagnosis was metastatic cancer
All of the above pathological entities may demonstrate the following radiologic features:
-
Mixed or low-density appearance showing areas of destruction
-
Irregular, invasive, permeative borders
-
“Moth-eaten” appearance
-
Periosteal reaction
-
Rapid growth
-
Possible paresthesia if they are present in the posterior mandible
The reported medical history, clinical examination, and the history of the present illness must always be applied to imaging findings to direct the most appropriate diagnosis. For example, if a medical history reveals that there was a previous episode of cancer, metastatic disease should always be included on the differential of conditions producing an ill-defined imaging presentation. Similarly, if the patient presents with clinical signs of inflammation, osteomyelitis may be the first choice. If there is a history of treatment with bisphosphonate medications, medically related osteonecrosis of the jaws should be considered.
3.6 Systemic, Metabolic, and Endocrine Disorders
Systemic, metabolic, and endocrine-related pathologic conditions may cause changes in the osseous tissues of the maxillofacial region depicted in CBCT studies. These changes are usually generalized rather than localized and not usually pathognomonic.
The most characteristic radiologic findings are those typically associated with osteoporosis which may present with wide bone marrow spaces or voids in the mandibular bone, thinning of the mandibular cortices and “moth-eaten appearance” of the mandibular cortices (Fig. 15.101). The association of certain radiological indices of the mandibular cortices and osteoporosis has been extensively reported in the literature (Horner et al. 2007; Devlin et al. 2007).

Reformatted panoramic (a) and a series of cross-sectional images (b) showing generalized thinning of the mandibular cortex, large voids in the cancellous component of the mandibular bone and a “moth-eaten” appearance. The imaging findings are consistent with osteoporosis of the mandible
Though not pathognomonic, certain hematologic disorders may present with radiologic findings in the jaws (Figs. 15.102 and 15.103).

Reformatted panoramic (a) and a series of cross-sectional images (b) of a patient diagnosed with sickle cell anemia. Note the generalized rarefaction of the mandible; however, this is not a distinctive feature of the disease

Reformatted panoramic (a) and a series of cross-sectional images (b) of a patient diagnosed with thalassemia illustrating generalized rarefaction of the mandible, however, this is not a distinctive feature of the disease
Endocrine disorders that may affect calcium balance nay present with radiologic findings in the jaws; hyperparathyroidism, although rarely, may cause marked changes in maxillary and mandibular bone, like brown tumors and osteomalacia (Fig. 15.104).

Reformatted thin panoramic (a) and a series of cross-sectional images (b) of a patient in chronic renal failure and secondary hyperparathyroidism. Note the extensive changes in the appearance of the maxillary and mandibular bones, with bicortical expansion and loss of bone density due to osteomalacia
References
Al-Moraissi EA, Pogrel MA, Ellis E 3rd (2016) Enucleation with or without adjuvant therapy versus marsupialization with or without secondary enucleation in the treatment of keratocystic odontogenic tumors: A systematic review and meta-analysis. J Craniomaxillofac Surg 44:1395–403
Bechara B, McMahan CA, Geha H, Noujeim M (2012) Evaluation of a cone beam CT artefact reduction algorithm. Dentomaxillofac Radiol 41:422–8
Chadwick JW, Alsufyani NA, Lam EW (2011) Clinical and radiographic features of solitary and cemento-osseous dysplasia associated simple bone cysts. Dentomaxillofac Radiol 40:230–235
Cheng J, Wang Y, Yu H, Wang D, Ye J, Jiang H, Wu Y, Shen G (2012) An epidemiological and clinical analysis of craniomaxillofacial fibrous dysplasia in a Chinese population. Orphanet J Rare Dis 7:80–86
Devlin H, Karayianni K, Mitsea A, Jacobs R, Lindh C, van der Stelt P, Marjanovic E, Adams J, Pavitt S, Horner K (2007) Diagnosing osteoporosis by using dental panoramic radiographs: the OSTEODENT project. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 104:821–828
Faitaroni LA, Bueno MR, Carvalhosa AA, Mendonça EF, Estrela C (2011) Differential diagnosis of apical periodontitis and nasopalatine duct cyst. J Endod 37:403–410
Gonzalez SM (2015) Describing radiographic lesions at: https://oralradiology.wordpress.com/describing-radiographic-lesions/. Accessed 6 Mar 2015
Horner K, Karayianni K, Mitsea A, Berkas L, Mastoris M, Jacobs R, Lindh C, van der Stelt P, Marjanovic E, Adams J, Pavitt S, Devlin H (2007) The mandibular cortex on radiographs as a tool for osteoporosis risk assessment: the OSTEODENT project. J Clin Densitom 10:138–146
Kaplan I, Nicolaou Z, Hatuel D, Calderon S (2008) Solitary central osteoma of the jaws: a diagnostic dilemma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 106:e22–e29
Kühl S, Walter C, Acham S, Pfeffer R, Lambrecht JT (2012) Bisphosphonate-related osteonecrosis of the jaws—a review. Oral Oncol 48:938–947
MacDonald D (2011) Oral and maxillofacial radiology: a diagnostic approach. Wiley-Blackwell, Hoboken, pp 1–39
MacDonald DS, Zhang L, Gu Y (2012) Calcification of the external carotid arteries and their branches. Dentomaxillofac Radiol 41:356–61.
MacDonald D, Gu Y, Zhang L, Poh C (2013) Can clinical and radiological features predict recurrence in solitary odontogenic keratocysts? Oral Surg Oral Med Oral Pathol Oral Radiol 115:263–271
MacDonald DS, Li TK, Goto TK (2015) A consecutive case series of nevoid basal cell carcinoma syndrome affecting the Hong Kong Chinese. Oral Surg Oral Med Oral Pathol Oral Radiol 120:408–15
MacDonald DS (2015a) Maxillofacial fibro-osseous lesions. Clin Radiol 70:25–36
MacDonald DS (2015b) A systematic review of the literature of nevoid basal cell carcinoma syndrome affecting East Asians and North Europeans. Oral Surg Oral Med Oral Pathol Oral Radiol 120:396–407
MacDonald D (2016) Lesions of the jaws presenting as radiolucencies on cone-beam CT. Clin Radiol71:972–85
MacDonald D (2017) Cone-beam computed tomography and the dentist. J Investig Clin Dent 8(1). doi: 10.1111/jicd.12178.
MacDonald-Jankowski DS (1995) Traumatic bone cysts in the jaws of a Hong Kong Chinese population. Clin Radiol 50:787–791
MacDonald-Jankowski DS (1999) Idiopathic osteosclerosis in the jaws of Britons and of the Hong Kong Chinese: radiology and systematic review. Dentomaxillofac Radiol 28:357–63
MacDonald-Jankowski DS (2004) Fibro-osseous lesions of the face and jaws. Clin Radiol 59:11–25
MacDonald-Jankowski DS, Li TK (2009) Fibrous dysplasia in a Hong Kong community: the clinical and radiological features and outcomes of treatment. Dentomaxillofac Radiol 38:63–72
MacDonald-Jankowski D (2009) Fibrous dysplasia: a systematic review. Dentomaxillofac Radiol 38:196–215
MacDonald-Jankowski DS (2010) Glandular odontogenic cyst: systematic review. Dentomaxillofac Radiol 39:127–139
Mathew R, Omami G, Gianoli D, Lurie A (2012) Unusual cone-beam computerized tomography presentation of traumatic (simple) bone cyst: case report and radiographic analysis. Oral Surg Oral Med Oral Pathol Oral Radiol 113:410–413
McDonnell D (1993) Dense bone island. A review of 107 patients. Oral Surg Oral Med Oral Pathol 76:124–128
Noffke CE, Raubenheimer EJ, MacDonald D (2012) Fibro-osseous disease: harmonizing terminology with biology. Oral Surg Oral Med Oral Pathol Oral Radiol 114:388–192
Rana RS, Wu JS, Eisenberg RL (2009) Periosteal reaction. AJR Am J Roentgenol 193:259–272
Rosenberg PA, Frisbie J, Lee J, Lee K, Frommer H, Kottal S, Phelan J, Lin L, Fisch G (2010) Evaluation of pathologists (histopathology) and radiologists (cone beam computed tomography) differentiating radicular cysts from granulomas. J Endod 36:423–428
Ruggieri P, Sim FH, Bond JR, Unni KK (1994) Malignancies in fibrous dysplasia. Cancer 73:1411–1424
Scarfe WC, Farman AG (2008) What is cone-beam CT and how does it work? Dent Clin N Am 52:707–30
Slootweg PJ (2006) Chapter 4. Maxillofacial bone and teeth. In: Cardesa A, Slootweg PJ (eds) Pathology of the head and neck. Springer, Heidelberg, pp 104–131
Speight P, Fantasia JE, Neville BW. (2017) Oodontogenic and non-odontogenic development cysts. In El-nagger AK, Chan JK, Grandis JR, Takata T, Slootweg PJ. (Eds.), WHO classification of head and neck tumours. 4th ed., Lyon: International Agency for research on Cancer. pp. 235–7
Suei Y, Taguchi A, Nagasaki T, Tanimoto K (2010) Radiographic findings and prognosis of simple bone cysts of the jaws. Dentomaxillofac Radiol 39:65–71
Suter VG, Büttner M, Altermatt HJ, Reichart PA, Bornstein MM (2011) Expansive nasopalatine duct cysts with nasal involvement mimicking apical le-sions of endodontic origin: a report of two cases. J Endod 37:1320–1326
Tortorici S, Amodio E, Massenti MF, Buzzanca ML, Burruano F, Vitale F (2008) Prevalence and distribution of odontogenic cysts in Sicily: 1986-2005. J Oral Sci 50:15–18
Treister NS, Friedland B, Woo SB (2010) Use of cone-beam computerized tomography for evaluation of bisphosphonate-associated osteonecrosis of the jaws. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 109:753–764
Uribe S, Rojas L, Rosas C (2013) Accuracy of imaging methods for detection of bone tissue invasion in patients with oral squamous cell carcinoma. Dentomaxillofac Radiol 42:20120346
Velez I, Siegel MA, Mintz SM, Rolle R (2010) The relationship between idiopathic bone cavity and orthodontic tooth movement: analysis of 44 cases. Dentomaxillofac Radiol 39:162–166
White S, Pharoah M (2009) Oral radiology: principles and interpretation, 7th edn. Mosby, St. Louis
Wright JM, Vered M (2017) Update from the 4th edition of the World Health Organization classification of head and neck tumours: odontogenic and maxillofacial bone tumors. Head Neck Pathol 11:68–77
Acknowledgments
Some figures are reproduced with permission from Wiley-Blackwell, the British Journal of Radiology and Elsevier (Clinical Radiology).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter
Cite this chapter
MacDonald, D., Angelopoulos, C., Scarfe, W.C. (2018). Cone Beam Computed Tomography and Maxillofacial Diagnosis. In: Scarfe, W., Angelopoulos, C. (eds) Maxillofacial Cone Beam Computed Tomography. Springer, Cham. https://doi.org/10.1007/978-3-319-62061-9_15
Download citation
DOI: https://doi.org/10.1007/978-3-319-62061-9_15
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-62059-6
Online ISBN: 978-3-319-62061-9
eBook Packages: MedicineMedicine (R0)