
Abstract
Background
Warfarin is an anticoagulant effective in preventing stroke, but it has a narrow therapeutic range requiring optimal adherence to achieve the most favorable effects.
Purpose
The goal of this study was to examine specific patient factors that might help explain warfarin non-adherence at outpatient anticoagulation clinics.
Method
In a prospective cohort study of 156 adults, we utilized logistic regression analyses to examine the relationship between the five Treatment Prognostics scales from the Millon Behavioral Medicine Diagnostic (MBMD), as well as three additional MBMD scales (Depression, Future Pessimism, and Social Isolation), and daily warfarin non-adherence assessed using electronic medication event monitoring systems caps over a median of 139 days.
Results
Four of the five Treatment Prognostic scales and greater social isolation were associated with warfarin non-adherence. When controlling for pertinent demographic and medical variables, the Information Discomfort scale remained significantly associated with warfarin non-adherence over time.
Conclusion
Although several factors were related to warfarin non-adherence, patients reporting a lack of receptivity to details regarding their medical illness seemed most at risk for warfarin non-adherence. This information might aid in the development of interventions to enhance warfarin adherence and perhaps reduce adverse medical events.
Similar content being viewed by others


Introduction
Warfarin is an anticoagulant commonly prescribed to prevent clotting among patients at risk for stroke or venous thromboembolism (VTE). The American College of Chest Physicians recommends the use of warfarin for stroke and VTE prophylactic therapy and regularly publishes guidelines for its effective utilization [1]. Warfarin is used routinely among patients experiencing atrial fibrillation (AF), a heart rhythm disturbance in which the upper chambers of the heart contract rapidly causing blood to accumulate, which can potentially lead to the formation of clots. In a large-scale meta-analysis of patients with AF, warfarin reduced the relative risk of stroke by 62% compared with placebo or control [2]. Warfarin has revolutionized the prevention of stroke among patients with AF, but it is by no means a panacea as many patients have International Normalized Ratio (INR) values (a measure of the degree of anticoagulation or blood thinning) out of the acceptable therapeutic range even in clinical trials [3–5]. Whereas under-anticoagulation on warfarin can lead to increased risk of recurrent VTE or stroke, over-anticoagulation may also lead to adverse events such as excessive bleeding and other hemorrhagic events sometimes resulting in death [6–10]. Thus, it is vital to determine the patient factors that underscore effective warfarin use to help prevent these types of adverse health outcomes.
There are numerous demographic and medical factors that can potentially complicate successful warfarin management. For example, diverse factors such as age, medical indication for warfarin, marital status, dietary regimen, drug–drug interactions [5, 11–17], and genetic factors [18–20] may alter the effects of warfarin. In addition to the difficulties of prescribing optimal dosages of warfarin in the face of these types of factors, physicians must also regularly monitor patient blood INR levels. INR levels in the range 2.0–3.0 is often the therapeutic goal of treatment and refers to the degree of anticoagulation necessary to maximize efficiency and minimize risk of adverse outcomes. However, because patients seldom maintain this narrow INR window, it is patient adherence to warfarin regimens that may be the largest determining factor of its effectiveness. A recent study found that patients had substantial difficulties maintaining adequate adherence with warfarin and that this poor adherence had a significant effect on anticoagulation control [21]. However, there are limited data on the patient attitudinal and behavioral factors that might help explain non-adherence among patients prescribed warfarin. There exists a wide range of potential influences on adherence behavior; patient factors are one such class of factors and are the main focus of this paper.
The purpose of the current study was to create an explanatory model of the association between attitudinal and behavioral factors and non-adherence to warfarin medication regimens over time utilizing a comprehensive assessment instrument, the Millon Behavioral Medicine Diagnostic (MBMD, [22]). The MBMD was developed specifically for medical patient populations and provides a broad assessment of patient adjustment to medical illness. The MBMD has been used effectively to explain medication adherence among HIV-positive men and women undergoing highly active antiretroviral therapy (HAART) over a 3-month period [23]. The current study, however, is the first to examine the MBMD in relation to warfarin adherence. We hypothesized that higher scores on the five MBMD Treatment Prognostics scales (Interventional Fragility, Medication Abuse, Information Discomfort, Utilization Excess, and Problematic Compliance), as well as higher scores on the MBMD Depression, Future Pessimism, and Social Isolation scales, would be associated with warfarin non-adherence over time.
Although psychosocial factors that impact medication adherence have been identified among patients with rheumatoid arthritis [24], cardiovascular disease [25, 26], cardiac rehabilitation patients [27], asthma patients [28, 29], renal dialysis patients [30, 31], HIV-infected individuals [32–36], and patients undergoing heart transplants [37], there is a dearth of studies examining these important factors among patients undergoing anticoagulation therapy. One recent study found that psychiatric illness, particularly substance abuse, was predictive of adverse medical outcomes during warfarin therapy, but adherence rates were not specifically studied [38]. Our group recently found that poorer general quality of life and cognitive impairment may also impact adherence to warfarin [39]. To date, however, there are no studies that have conducted a comprehensive evaluation of the psychosocial, attitudinal, and behavioral factors that might impact warfarin adherence.
The key psychosocial factors that have consistently emerged within the adherence literature as associated with poorer adherence are higher depressive symptoms, greater pessimism versus optimism, and perceived lack of social support. For example, greater depressive symptoms are associated with poorer adherence to antihypertensive medications among people at risk for or diagnosed with cardiovascular disease [25, 26]. Greater pessimism or lower optimism is related to poorer adherence to anti-psychotic medications [40], less optimal adherence to psoriasis treatment regimens [41], and poorer adherence to highly active antiretroviral therapy among people with HIV/AIDS [42]. Lower perceived social support is also related to lower HAART adherence as well [43]. As mentioned above, the impact of these important psychosocial factors on adherence are understudied among patients undergoing warfarin management.
In addition to a lack of understanding of the patient factors that might help explain warfarin non-adherence, there is also scant information available about objective adherence levels among patients prescribed warfarin. It is difficult to quantify adherence behavior on a daily basis, as patients frequently overestimate their medication compliance [44–47]. Utilizing daily electronic pill cap monitoring of warfarin non-adherence is a method considered one of the most objective means of measuring medication adherence [48], and we have found in a prior study that medication event monitoring systems (MEMS) caps are an effective method of assessing warfarin adherence [44]. Furthermore, assessing patients within an anticoagulation clinic may also provide an opportunity to quantify adherence behavior within a controlled and uniform environment.
The overarching aim of this study was to determine if the MBMD, a psychological battery tapping multiple patient factors, administered early in the treatment process can successfully identify attitudinal and behavioral risk factors of warfarin non-adherence. A better understanding of patient factors that explain non-adherence to warfarin may help identify those patients in need of adherence counseling and also perhaps aid in the development of interventions that might reduce medical complications and optimize warfarin therapy.
Methods
Participants
The current study was part of a larger prospective cohort study, the International Normalized Ratio Adherence and Genetics (IN-RANGE) component of the Program for the Reduction in Medication Errors (PRIME) study (PRIME IN-RANGE study). The primary aim of the current study was to examine the utility of the MBMD to predict warfarin adherence. As part of this parent project, we recruited participants through two specialized anticoagulation clinics: the Hospital of the University of Pennsylvania (HUP) in Philadelphia and the Philadelphia Veterans Affairs Medical Center (PVAMC). The institutional review boards at both participating hospitals approved the study, and all of the participants provided informed, written consent to participate. A full description of our inclusion/exclusion criteria is provided elsewhere [21]. Briefly, patients were eligible for participation if they were at least 21 years old and were also within 2 months of their initiation of anticoagulation therapy with a target INR of 2.0 to 3.0.
Procedures
A research nurse or other trained study personnel approached all patients meeting the screening criteria for inclusion in the study, and informed consent was obtained from those interested in participating prior to their inclusion in the study. We then obtained demographic (e.g., age, gender, race, education, marital status), medical (e.g., indication for warfarin, co-morbid medical conditions, other medication usage), and health behavior (e.g., nicotine use, alcohol use) information at study entry via self-report. As part of the parent project, participants also completed other measures distinct and separate from the MBMD, including measures of cognitive functioning, general quality of life, healthcare utilization, and general health behaviors. These measures are distinctly different from the constructs assessed through the MBMD, and the primary aim of the current study was to examine the value of the MBMD in predicting adherence. If patients were unable to complete the MBMD at their initial visit, they were allowed to complete it at home and return it on their next clinic visit.
Medication Adherence
The main outcome measure in this study was adherence to warfarin as measured daily during the course of the study using electronic medication event monitoring systems pill caps (MEMS caps, AARDEX, Zug, Switzerland), an electronic device that captures the date and time of every instance patients open their medication container or pill bottle. We assessed a dichotomous outcome of adherence versus non-adherence on a daily basis across the study period. Additionally, in a sub-analysis, we also classified the patients as early adherers versus late adherers over the study period to see if early or late adoption of the warfarin regimen or perhaps regimen fatigue or burnout was evident. This categorization was accomplished by collapsing visits into early versus late based on the median follow-up time and dichotomizing incorrect adherence at 20%. For those participants who used standard pharmacy pill bottles for warfarin storage, we fitted the MEMS caps directly onto their pill bottles at the start of the study. If any participants used weekly pill reminder boxes to store their medications, we provided them with empty pill bottles with a MEMS cap attached and instructions on how to open and close the MEMS cap bottle each time they took their warfarin from the pill box. In these situations, the MEMS cap functioned as a diary of daily warfarin use. All patients brought their MEMS caps on each return visit to their clinic, and adherence data were downloaded at that time.
In this study, we defined non-adherence as either failure to activate a MEMS cap in a 24-h period or activating a MEMS cap more than once in a 24-h period. Because warfarin was always prescribed once per day, we were able to categorize each patient as either adherent or non-adherent on a daily basis. Because both skipped doses and extra doses may result in INR instability and adverse outcomes and also because activation of MEMS caps more than once in a 24-h period was relatively rare compared to just skipped doses [21], these events were not evaluated separately. All patients were followed for the duration of their warfarin therapy or until the end of the study period. Some patients on warfarin require only a few weeks of treatment, but some require several months of treatment, so a relatively high degree of variability in the duration of follow-up days was expected in this study.
The Millon Behavioral Medicine Diagnostic
The Millon Behavioral Medicine Diagnostic [22] is a self-report inventory designed to assess a wide array of psychosocial and behavioral factors that impact adjustment to illness and medical treatment outcomes. The main sections of the MBMD include: (1) Psychiatric Indications; (2) Coping Styles; (3) Stress Moderators; (4) Treatment Prognostics; and (5) Management Guides. The MBMD contains 165 true/false items and takes approximately 20–30 min to complete. The MBMD was validated on a heterogeneous sample of over 700 medical patients, ages 18 to 85, with a variety of conditions, including heart disease, cancer, diabetes, chronic pain, and HIV/AIDS [22]. The normative study found that the MBMD was both internally reliable (internal consistency coefficients mean α for all scales = 0.79) and consistent (test–retest reliability mean for all scales = 0.83). In addition, the MBMD was also associated with a variety of other individual measures that assess similar constructs and demonstrated very good convergent validity in the normative study.
The MBMD is computer scored, generating a profile of scores that are automatically corrected for the patients' response styles (i.e., over-reporting or under-reporting symptoms). Each MBMD scale is represented by a raw score that is also converted to a prevalence score, which reflects the participant's position on that construct compared to the normative sample. A prevalence score of 75 or higher is considered clinically significant [22]. Because the prevalence scores are not linear, the raw scores from the MBMD, which are linear, were employed in our explanatory models to make use of parametric statistics. Prior research with the MBMD and comparable tests has also successfully employed raw scores for similar reasons [23, 49].
In the current study, we focused our attention on the Treatment Prognostics scales (Interventional Fragility, Medication Abuse, Information Discomfort, Utilization Excess, and Problematic Compliance) in an explanatory model of warfarin non-adherence because these scales were specifically designed to identify behavioral and attitudinal aspects of a patient's life that may complicate treatment efficacy. The MBMD Treatment Prognostic indicators were selected because they were developed specifically to assess long-standing attitudinal and behavioral aspects of a patient's life that may complicate treatment efficiency. The Interventional Fragility scale assesses whether patients will be able to adjust emotionally to the demands of physically and psychologically stressful medical protocols; the Medication Abuse scale assesses the likelihood that patients will have problems with or will misuse medication; the Information Discomfort scale assesses patients' lack of receptivity to specific details about diagnostic, prognostic, and treatment procedures and outcomes; the Utilization Excess scale assesses the likelihood that patients will use medical services more than the average patient with a similar medical condition; the Problematic Compliance scale assesses whether patients will inadvertently or intentionally resist following medical recommendations [22].
We also examined several psychosocial factors in addition to the five MBMD Treatment Prognostic factors. As noted above, three key psychosocial factors, depressive symptoms, greater pessimism versus optimism, and lack of social support utilization, have consistently emerged within the adherence literature as significantly associated with poorer adherence, so we also specifically examined the MBMD Depression, Future Pessimism, and Social Isolation subscales as indicators of these psychosocial factors in relation to warfarin non-adherence as well.
Statistical Analyses
We utilized multivariable logistic regression for longitudinal data using generalized estimating equations models with an independent working correlation matrix, as employed in SAS GENMOD (SAS Institute, Cary, N.C., version 9.1). The working correlation matrix was governed by procedures outlined for examining longitudinal models with time-varying factors [50]. Non-adherence to warfarin was the dependent variable in all the primary analyses. The number of patient days on warfarin was chosen as the unit of analysis to maximize statistical power to detect risk factors related to daily use. This procedure accounted for the lack of independence of adherence estimates due to repeated measurements within subjects and for the varying contributions of follow-up time period per patient. Prior to conducting our main analyses, we determined the degree of association between our predictors and also the internal consistency (using alpha coefficients) for these scales as well.
Unadjusted logistic regression models associating warfarin non-adherence with the raw subscale scores on the five Treatment Prognostic scales, as well as the MBMD Depression, Social Isolation, and Future Pessimism scales, were initially examined. The level of association in all of these initial models was quantified using beta weights and 95% confidence intervals (95% CI) and odds ratios (OR) and 95% CI. Based on our earlier work [39] and also a review of the demographic and medical variables related to warfarin adherence [5, 11–17], we then constructed a stringent baseline model consisting of the following seven potentially confounding factors: age, gender, race, indication for warfarin, education, marital status, and clinic site. These variables were either significantly associated with warfarin adherence (p < 0.05) in the current analyses or were known to be important factors of warfarin adherence based on the literature in this area. Logistic regression models associating warfarin non-adherence with the raw subscale scores on the five MBMD Treatment Prognostic scales, as well as the MBMD Depression, Social Isolation, and Future Pessimism scales adjusted for this baseline model were then examined. Only those scales significantly associated with warfarin adherence after controlling for this baseline model were considered further for inclusion in a final explanatory model.
In a sub-analysis, we compared early versus late adherers on each of the eight MBMD scales under investigation using analysis of variance models and Scheffe's test for multiple comparisons.
Results
Participants
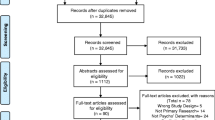
Of the 292 patients approached for the study, 101 refused to utilize MEMS caps for their medication usage and were thus excluded from the current study. Of the remaining 191 subjects with MEMS adherence data, we obtained complete and valid demographic, medical, and MBMD data on 156 of the 191 patients (82%). A comparison of the final sample of participants with complete MBMD and MEMS caps warfarin adherence data (n = 156) with those who refused MEMS caps or had incomplete data showed no differences in age (p = 0.12), gender (p = 0.15), race (p = 0.65), indication for warfarin (p = 0.46), marital status (p = 0.96), clinic site (p = 0.31), and employment status (p = 0.25). The only significant difference observed was for education level, with the completers reporting a greater education level than non-completers (p < 0.009). Of the 156 patients, 102 (65%) were recruited from the HUP clinic and 54 (35%) from the VA clinic.
Demographic and Medical Characteristics
Demographic and medical characteristics are presented in Table 1. Among the 156 participants, the average age was 55.8 (SD = 14.8) years, and 64% were men. The majority were African–American (53%) or Caucasian (44%). Sixty-three percent reported an education level beyond high school. The majority (32%) were currently employed, although a sizeable percentage of participants were retired (30%) or disabled (25%). The majority (92%) were insured through private insurance, Medicare, or through VA benefits. Medical indication for warfarin was primarily due to atrial fibrillation/atrial flutter (40%) or deep vein thrombosis/pulmonary embolism (40%). The vast majority of participants (84%) reported visiting their primary care physician in the past year, and the mean number of baseline medications was 5.8 (SD = 4.0). The majority of participants (84%) reported zero alcoholic beverages consumed over the past week, and only 16% of the sample was currently smoking cigarettes.
Adherence to Warfarin
The 156 participants were followed while undergoing anticoagulation for a median of 139 days. Warfarin non-adherence occurred in 6,443 of 29,022 (22% of total) patient days observed. The 35 subjects who were not included in the analyses due to failure to complete the MBMD or incomplete demographic data had a similar rate of non-adherence (20% versus 22% of patient days observed, p = 0.27) as the completers. In our sub-analysis of categorizing early versus late adherence, we found that the majority of participants (76%) were either consistently adherent or non-adherent across the study period (44% of participants were adherent both early and late during the follow-up period; 32% of participants were non-adherent both early and late during the follow-up period). We found that 15% of participants were early adherers and 9% were late adherers, and there were no significant differences between patients categorized as consistent versus inconsistent or early versus later adherers on any of the eight MBMD scales under investigation (all p values >0.05).
Millon Behavioral Medicine Diagnostic
Descriptive statistics for the overall MBMD are depicted in Table 2. Seventeen patients (11%) fully completed the MBMD at the clinic site, whereas 139 patients (89%) started the MBMD at their clinic visit and completed it at home. There were no significant differences between those completing the MBMD at the clinic versus those completing the MBMD at home on the MBMD subscales under investigation (all p values >0.05). Within each of the main sections of the MBMD, the clinical scales with the highest prevalence scores were as follows: Psychiatric Indications: Depression (22%); Coping Styles: Respectful (26%); Stress Moderators: Functional Deficits (31%); Treatment Prognostics: Problematic Compliance (33%); and Management Guides: Adjustment Difficulties (36%). When we examined our MBMD predictors to determine their degree of association, Pearson r's ranged from −0.03 (p = 0.74) to 0.88 (p < 0.001), which are values similar to those observed in the MBMD validation study [22]; average internal consistency alpha coefficients for the MBMD predictors in the current study were also similar to those observed in the MBMD validation study [22]. Overall, there was considerable variability in the presence of psychiatric difficulties, different coping styles, stress moderators, and treatment prognostic factors among the outpatient clinic sample.
Associations between the MBMD Treatment Prognostics Scales and Warfarin Non-adherence
Results of both the unadjusted and adjusted logistic regression models associating non-adherence to warfarin and raw scores on the five MBMD Treatment Prognostics indicators are presented in Table 3. Higher scores on four of the five Treatment Prognostics scales, Interventional Fragility (β = 0.030, 95% CI (0.003/0.057); OR = 1.03, 95% CI (1.00–1.06), p = 0.031), Medication Abuse (β = 0.051, 95% CI (0.004/0.097); OR = 1.05, 95% CI (1.00–1.10), p = 0.032), Information Discomfort (β = 0.122, 95% CI (0.038/0.207); OR = 1.13, 95% CI (1.04–1.23), p = 0.005), Utilization Excess (β = 0.037, 95% CI (0.011/0.063); OR = 1.04, 95% CI (1.01–1.06), p = 0.005), and on the MBMD Social Isolation scale (β = 0.022, 95% CI (0.003/0.041); OR = 1.02, 95% CI (1.00–1.04), p = 0.026) were significantly associated with non-adherence to warfarin sodium. After controlling for the baseline model of demographic and medical variables (age, gender, race, indication for warfarin, education, marital status, and clinic site), higher scores on the MBMD Information Discomfort scale remained significantly associated with warfarin non-adherence (β = 0.105, 95% CI (0.022/0.188); OR = 1.11 (95% CI (1.02–1.21), p = 0.013).
Discussion
In this study, we examined the association between several specific patient factors and warfarin non-adherence among 156 adults treated at two outpatient anticoagulation clinics. We utilized the MBMD, which was specifically developed for medical patient populations to provide a thorough evaluation of patient functioning and adjustment to illness. In addition, to capture medication adherence more objectively and uniformly, we utilized daily MEMS caps readings collected over a median of 139 days within a structured outpatient clinic setting.
Warfarin non-adherence was common in our outpatient sample, occurring in 22% of total patient days observed. As hypothesized, we found that four of the five Treatment Prognostics scales (Interventional Fragility, Medication Abuse, Information Discomfort, and Utilization Excess), as well as higher scores on the MBMD Social Isolation scale were significantly associated with warfarin non-adherence. Similar to other work utilizing these scales of the MBMD to explain adherence to HAART medication among HIV-positive men and women [23], the MBMD Medication Abuse scale was also useful in identifying risk of warfarin non-adherence. However, unlike in the HIV study [23], the Medication Abuse scale was not related to non-adherence once we controlled for pertinent demographic and medical variables included in the baseline model. This supports the notion that attitudinal and behavioral factors associated with non-adherence may vary based on specific health actions required to obtain optimal adherence. Interestingly, the Problematic Compliance scale was the only MBMD Treatment Prognostics scale that was not associated with warfarin non-adherence, and this was also the case in the HIV study noted above [23]. This scale identifies a disinclination to follow home-care advice, to adhere to nutritional instructions or change diet, and to maintain physician appointments [22]. Thus, the lack of association with the Problematic Compliance scale and adherence behavior in the current study is most likely due to the fact that this scale assesses a more diverse range of compliance issues rather than on focused medication adherence behavior (i.e., pill-taking).
Although four of five of the MBMD Treatment Prognostics scales and one of the three additional key MBMD psychosocial scales (Social Isolation) examined were associated with warfarin non-adherence in our study, only the Informational Discomfort scale was associated with warfarin non-adherence when controlling for the baseline model of seven demographic and medical variables. Specifically, patients acknowledging a greater sensitivity to illness-related information from physicians and a lack of receptivity to details regarding medical illness seem most at risk of warfarin non-adherence even when controlling for a wide array of potentially confounding medical and demographic factors. Our analyses demonstrate that each one-point increase in MBMD Information Discomfort scale is associated with an 11% reduction in the risk of non-adherence in the sample. Prior work by our team found that for each 10% increase in non-adherence to warfarin there is a 14% increase in the risk of under-anticoagulation, which can have devastating adverse health consequences, such as increased risk of thromboembolism among post-operative patients and significantly higher rates of morbidity and mortality among stroke patients [21]. Thus, we feel that this main finding is not only statistically significant but also clinically meaningful as well. Based on the results of this study, the Information Discomfort scale may perhaps help identify medical patients with warfarin adherence problems early in the course of treatment. The Information Discomfort scale asks questions such as, “I'd rather not know the details of an illness I might have” and “I don't want my doctor to review with me the results of all my medical tests.” Thus, this MBMD Treatment Prognostics scale might be employed in anticoagulation clinic settings where it may be important to identify patient attitudes and behaviors indicative of reluctance to hear information about their medical information and treatments.
The strengths of this study are the prospective design, comprehensive evaluation of psychosocial functioning, and the objective and uniform assessment of adherence using MEMS cap data within a controlled clinic environment. However, there were also some limitations of the study as well. First, although the MBMD assesses a wide array of individual patient factors that may be important in determining adherence, we focused our attention a priori only on the five Treatment Prognostics scales and three additional psychosocial scales. We did so because these scales were specifically developed to identify long-standing behavioral and attitudinal patterns that may complicate treatment efficacy or have been associated with adherence in prior research, and also to reduce our statistical tests and thus type I error in this study. However, it is possible that some other important factors not assessed by the MBMD (e.g., patients' insight into their illness, sleep quality, doctor–patient communication patterns, specific adherence behavioral skills) may have also impacted warfarin adherence and should be examined in future studies. Second, the use of MEMS caps to measure adherence raised logistical challenges as many patients originally recruited refused to use them. However, we found no significant differences in the demographic and medical factors between the MEMS caps refusers and those who opted to use the MEMS caps except for education level, which was controlled for in the baseline model. Although we did not find any significant differences in our results between these two groups and our prior work has also shown no differences between adherence and level of anticoagulation control between these two groups [21], it is possible that there may be yet undetected differences among those using the MEMS caps directly on their warfarin bottles versus those using MEMS caps as a daily diary. It is also important to note that MEMS caps do not provide a perfect indication of adherence behavior and that some patients may also find them complicated to use. Third, it is possible that our study findings, although derived from subjects recruited from two different centers (a university hospital and a VA hospital), may not generalize to other clinics and among individual physician practices, in particular anticoagulation management outside of specialized clinics. Further research is needed at other clinic settings and among individual physician practices to confirm these findings. In addition, future studies should consider devising a cost index associated with warfarin non-adherence or perhaps evaluate morbidity data through chart review in relation to patient factors implicated in poor anticoagulation control. This future work would also benefit by employing more advanced statistical techniques with larger patient samples to better discern patient adherent versus non-adherent groups.
The results of this study may have a number of clinical implications. Although healthcare providers can usually take the necessary action of better informing patients of what can happen if medications are not taken as prescribed, providing basic information may not be enough. As our results show, non-adherent patients may be reluctant to hear this type of information based on their heightened degree of sensitivity to medical information. Several published studies have examined medication beliefs and barriers to warfarin adherence [12, 51–53], but to our knowledge, there are no published studies that have evaluated a patient's general trait sensitivity to medical information in association with warfarin non-adherence, and this may be a relevant patient factor to assess in this domain. In addition, patients' level of health literacy and also any miscommunication between patients and physicians needs to be taken into consideration, as these are factors that may affect patient attitudes and alter anticoagulant-related health outcomes [54, 55] and which also have been associated with adherence in HIV-infected patients [56, 57]. Emerging intervention strategies utilizing videos depicting physician–patient dialogues about warfarin were effective in educating patients about anticoagulant medication and had a positive impact on their beliefs [58]. Future work may further assess for and perhaps develop intervention strategies aimed at addressing long-standing beliefs, abilities, and attitudinal patterns early on in the course of warfarin medication regimens to help optimize adherence.
References
Hirsh J, Guyatt G, Albers GW, Schünemann HJ. The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy: evidence-based guidelines. Chest. 2004;126:172S–3S.
No authors listed. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation: analysis of pooled data from five randomized controlled trials. Arch Intern Med. 1994;154:1449-57.
The European Atrial Fibrillation Trial Study Group. Optimal oral anticoagulant therapy in patients with nonrheumatic atrial fibrillation and recent cerebral ischemia. N Engl J Med. 1995;333:5–10.
Samsa GP, Matchar DB, Goldstein LB, et al. Quality of anticoagulation management among patients with atrial fibrillation: results of a review of medical records from 2 communities. Arch Intern Med. 2000;160:967–73.
Wittkowsky AK, Devine EB. Frequency and causes of overanticoagulation and underanticoagulation in patients treated with warfarin. Pharmacotherapy. 2004;24:1311–6.
Hylek EM, Skates SJ, Sheehan MA, Singer DE. An analysis of the lowest effective intensity of prophylactic anticoagulation for patients with nonrheumatic atrial fibrillation. N Engl J Med. 1996;335:540–6.
Hylek EM, Singer DE. Risk factors for intracranial hemorrhage in outpatients taking warfarin. Ann Intern Med. 1994;120:897–902.
Gitter MJ, Jaeger TM, Petterson TM, Gersh BJ, Silverstein MD. Bleeding and thromboembolism during anticoagulant therapy: a population-based study in Rochester, Minnesota. Mayo Clin Proc. 1995;70:725–33.
Fihn SD, Callahan CM, Martin DC, McDonell MB, Henikoff JG, White RH. The risk for and severity of bleeding complications in elderly patients treated with warfarin. Ann Intern Med. 1996;124:970–9.
Palareti G, Leali N, Coccheri S, et al. Bleeding complications of oral anticoagulant treatment: an inception-cohort, prospective collaborative study (ISCOAT). Italian Study on Complications of Oral Anticoagulant Therapy. Lancet. 1996;348:423–8.
Inoue H, Nozawa T, Hirai T, et al. Accumulation of risk factors increases risk of thromboembolic events in patients with nonvalvular atrial fibrillation. Circ J. 2006;70:651–6.
Orensky IA, Holdford DA. Predictors of noncompliance with warfarin therapy in an outpatient anticoagulation clinic. Pharmacotherapy. 2005;25:1801–8.
York M, Agarwal A, Ezekowitz M. Physicians' attitudes and the use of oral anticoagulants: surveying the present and envisioning future. J Thromb Thrombolysis. 2003;16:33–7.
Lynch T, Price A. The effect of cytochrome P450 metabolism on drug response, interactions, and adverse effects. Am Fam Physician. 2007;76:391–6.
Hirsh J, Dalen J, Anderson DR, et al. Oral anticoagulants: mechanism of action, clinical effectiveness, and optimal therapeutic range. Chest. 2001;119:8S–21.
Garcia D, Regan S, Crowther M, Hughes RA, Hylek EM. Warfarin maintenance dosing patterns in clinical practice: implications for safer anticoagulation in the elderly population. Chest. 2005;127:2049–56.
Palareti G, Legnani C, Guazzaloca G, et al. Risks factors for highly unstable response to oral anticoagulation: a case-control study. Br J Haematol. 2005;129:72–8.
Kealey C, Chen Z, Christie J, et al. Warfarin and cytochrome P450 2C9 genotype: possible ethnic variation in warfarin sensitivity. Pharmacogenomics. 2007;8:217–25.
Higashi MK, Veenstra DL, Kondo LM, et al. Association between CYP2C9 genetic variants and anticoagulation-related outcomes during warfarin therapy. JAMA. 2002;287:1690–8.
Muszkat M, Blotnik S, Elami A, Krasilnikov I, Caraco Y. Warfarin metabolism and anticoagulant effect: a prospective, observational study of the impact of CYP2C9 genetic polymorphism in the presence of drug–disease and drug–drug interactions. Clin Ther. 2007;29:427–37.
Kimmel SE, Chen Z, Price M, et al. The influence of patient adherence on anticoagulation control with warfarin: results from the International Normalized Ratio Adherence and Genetics (IN-RANGE) Study. Arch Intern Med. 2007;167:229–35.
Millon T, Antoni M, Millon C, Meagher S, Millon GS, Diagnostic BM. Millon Behavioral Medicine Diagnostic. Minneapolis: NCS Assessments; 2001.
Cruess DG, Minor S, Antoni MH, Millon T. Utility of the Millon Behavioral Medicine Diagnostic (MBMD) to predict adherence to highly active antiretroviral therapy (HAART) medication regimens among HIV-positive men and women. J Pers Assess. 2007;89:277–90.
Wong M, Mulherin D. The influence of medication beliefs and other psychosocial factors on early discontinuation of disease-modifying anti-rheumatic drugs. Musculoskelet Care. 2007;5:148–59.
Bane C, Hughes CM, McElnay JC. The impact of depressive symptoms and psychosocial factors on medication adherence in cardiovascular disease. Patient Educ Couns. 2006;60:187–93.
Wang PS, Bohn RL, Knight E, Glynn RJ, Mogun H, Avorn J. Noncompliance with antihypertensive medications: the impact of depressive symptoms and psychosocial factors. J Gen Intern Med. 2002;17:504–11.
Hershberger PJ, Robertson KB, Markert RJ. Personality and appointment-keeping adherence in cardiac rehabilitation. J Cardpulm Rehabil. 1999;19:106–11.
Barton C, Clarke D, Sulaiman N, Abramson M. Coping as a mediator of psychosocial impediments to optimal management and control of asthma. Respir Med. 2003;97:747–61.
Bender B, Milgrom H, Rand C, Ackerson L. Psychological factors associated with medication nonadherence in asthmatic children. J Asthma. 1998;35:347–53.
Christensen AJ, Smith TW. Personality and patient adherence: correlates of the five-factor model in renal dialysis. J Behav Med. 1995;18:305–13.
Cummings KM, Becker MH, Kirscht JP, Levin NW. Psychosocial factors affecting adherence to medical regiments in a group of hemodialysis patients. Med Care. 1982;20:567–80.
Carrieri MP, Leport C, Protopopescu C, et al. Factors associated with nonadherence to highly active antiretroviral therapy: a 5-year follow-up analysis with correction for the bias induced by missing data in the treatment maintenance phase. J Acquir Immune Defic Syndr. 2006;41:477–85.
Halkitis PN, Kutnick AH, Slater S. The social realities of adherence to protease inhibitor regimens: substance use, health care and psychological states. J Health Psychol. 2005;10:545–58.
Naar-King S, Arfken C, Frey M, Harris M, Secord E, Ellis D. Psychosocial factors and treatment adherence in paediatric HIV/AIDS. AIDS Care. 2006;18:621–8.
Tucker JS, Orlando M, Burnam MA, Sherbourne CD, Kung FY, Gifford AL. Psychosocial mediators of antiretroviral nonadherence in HIV-positive adults with substance use and mental health problems. Health Psychol. 2004;23:363–70.
Weaver K, Llabre M, Durán RE, et al. A stress and coping model of medication adherence and viral load in HIV+ men and women on highly active antiretroviral therapy. Health Psychol. 2005;24:385–92.
Chacko RC, Harper RG, Kunik M, Young J. Relationship of psychiatric morbidity and psychosocial factors in organ transplant candidates. Psychosomatics. 1996;37:100–7.
Schauer DP, Moomaw CJ, Wess M, Webb T, Eckman MH. Psychosocial risk factors for adverse outcomes in patients with nonvalvular atrial fibrillation receiving warfarin. J Gen Intern Med. 2005;20:1114–9.
Platt AB, Localio AR, Brensinger CM, et al. Risk factors for nonadherence to warfarin: results from the IN-RANGE study. Pharmacoepidemiol Drug Saf. 2008;17:853–60.
Bryne MK, Deane FP, Caputi P. Mental health clinicians' beliefs about medicines, attitudes, and expectations of improved medication adherence in patients. Evauation & the Health Professions. 2008;31:390–403.
Richards HL, Fortune DG, Griffiths CE. Adherence to treatment in patients with psoriasis. J Eur Acad Dermatol Venereol. 2006;20:370–9.
Holmes WC, Pace JL. HIV-seropositive individuals' optimistic beliefs about prognosis and relation to medication and safe sex adherence. J Gen Intern Med. 2002;17:677–83.
Gonzalez JS, Penedo FJ, Antoni MH, Durán RE, McPherson-Baker S, Ironson G, et al. Social support, positive states of mind, and HIV treatment adherence in men and women living with HIV/AIDS. Health Psychol. 2004;23:413–8.
Parker CS, Chen Z, Price M, et al. Adherence to warfarin assessed by electronic pill caps, clinician assessment, and patient reports: results from the IN-RANGE Study. J Gen Intern Med. 2007;22:1254–9.
Urquhart J. Variable compliance and persistence with prescribed drug dosing regimens: implications for benefits, risks and economics of pharmacotherapy. In: Strom BL, editor. Pharmacoepidemiology. 4th ed. John Wiley & Sons, Ltd.; 2005. p. 767-789.
Burnier M, Schneider MP, Chiolero A, Stubi CL, Brunner HR. Electronic compliance monitoring in resistant hypertension: the basis for rational therapeutic decisions. J Hypertens. 2001;19:335–41.
Waeber B, Burnier M, Brunner HR. Compliance with antihypertensive therapy. Clin Exp Hypertens. 1999;21:973–85.
Choo PW, Rand CS, Inui TS, et al. Validation of patient reports, automated pharmacy records, and pill counts with electronic monitoring of adherence to antihypertensive therapy. Med Care. 1999;37:846–57.
Byrnes DM, Antoni MH, Goodkin K, et al. Stressful events, pessimism, natural killer cell cytotoxicity, and cytotoxic/suppressor T cells in HIV+ black women at risk for cervical cancer. Psychosom Med. 1998;60:714–22.
Pepe MS, Anderson GA. A cautionary note on inference for marginal regression models with longitudinal data and general correlation response data. Commun Stat Simul Comput. 1994;23:939–51.
Davis NJ, Billett HH, Cohen HW, Arnsten JH. Impact of adherence, knowledge, and quality of life on anticoagulation control. Ann Pharmacother. 2005;39:632–6.
Nadar S, Begum N, Kaur B, Sandhu S, Lip GY. Patients' understanding of anticoagulant therapy in a multiethnic population. J R Soc Med. 2003;96:175–9.
Lip GY, Chin BS, Prasad N. ABC of antithrombotic therapy: antithrombotic therapy in myocardial infarction and stable angina. BMJ. 2002;325:1287–9.
Fang MC, Machtinger EL, Wang F, Schillinger D. Health literacy and anticoagulation-related outcomes among patients taking warfarin. J Gen Intern Med. 2006;21:841–6.
Schillinger D, Machtinger EL, Wang F, Palacios J, Rodriguez M, Bindman A. Language, literacy, and communication regarding medication in an anticoagulation clinic: a comparison of verbal vs. visual assessment. J Health Commun. 2006;11:651–64.
Kalichman SC, Amaral CM, Stearns H, et al. Adherence to antiretroviral therapy assessed by unannounced pill counts conducted by telephone. J Gen Intern Med. 2007;22:1003–6.
Graham J, Bennett IM, Holmes WC, Gross R. Medication beliefs as mediators of the health literacy-antiretroviral adherence relationship in HIV-infected individuals. AIDS Behav. 2007;11:385–92.
Mazor KM, Baril J, Dugan E, Spencer F, Burgwinkle P, Gurwitz JH. Patient education about anticoagulant medication: is narrative evidence or statistical evidence more effective? Patient Educ Couns. 2007;69:145–57.
Acknowledgments
This study was supported by grants from the National Institutes of Health (NIH, R01-HL66176) and the Agency for Healthcare Research and Quality (AHRQ, P01-HS11530). Dr. Kimmel was also supported by NIH Grant K24HL070936.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cruess, D.G., Localio, A.R., Platt, A.B. et al. Patient Attitudinal and Behavioral Factors Associated with Warfarin Non-adherence at Outpatient Anticoagulation Clinics. Int.J. Behav. Med. 17, 33–42 (2010). https://doi.org/10.1007/s12529-009-9052-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-009-9052-6