
Abstract
Background
Since January 1st, 2005, the current situation for bariatric surgery has been examined by means of a voluntary quality assurance study in Germany with a multicenter design in which 38 hospitals and surgical departments participated. The data are registered in cooperation with the Institute of Quality Assurance in Surgery at the Otto-von-Guericke University of Magdeburg (Germany).
Methods
Data describing peri-interventional characteristics were prospectively documented in an internet online data registry. All primary bariatric procedures performed since January 1st, 2005, were registered. In addition, reoperations in patients who had previously undergone primary surgical intervention were included. As a representative excerpt from the overall prospective multicenter observational study on obesity surgery, data on the type, regimen, and time course of deep venous thrombosis (DVT) prophylaxis were documented. From the number and spectrum of complications, the incidences of clinically manifest DVT or pulmonary embolism (PE) were derived during the in-hospital course and follow-up in conjunction with the type of surgical procedure and body mass index (BMI).
Results
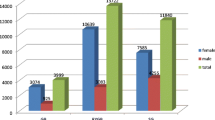
Overall, 3,122 bariatric procedures were performed at 38 German hospitals between January 2005 and December 2007. These procedures were subdivided into 2,869 primary operations and 253 revisions (sex ratio, male to female = 25.6:74.4%). The average BMI of all patients was 48.5 kg/m² in 2005, 48.4 kg/m² in 2006, and 48.0 kg/m² in 2007. In 2005 and 2006, gastric banding (GB) was the most commonly performed operation, followed by Roux-en-Y gastric bypass (RYGBP). In 2007, RYGBP was carried out in 42.1% of all bariatric procedures. Interestingly, the incidence of deep venous thrombosis (DVT) was only 0.06%, whereas PE occurred in 0.06% of patients only after hospital discharge. The DVT prophylaxis protocol used has been changed for the last 2 years: the majority of patients with a BMI above 50 kg/m² received low-molecular-weight heparin twice a day.
Conclusion
In Germany, a trend from GB to sleeve gastrectomy (SG) and malabsorptive approach has been evaluated. This trend is associated with differences of the DVT prophylaxis regimen in the profile of bariatric surgical patients depending on BMI and the type of bariatric procedure. Despite the low incidence of DVT and pulmonary embolism (PE) detected, there is a lack of evidence on a reasonable regimen for sufficient DVT prophylaxis in bariatric surgery; instead, there are only recommendations from the guidelines and statements of a specific medical society. Therefore, prospective studies are necessary to determine the optimal DVT prophylaxis for bariatric surgical patients as well as obese patients undergoing surgery.
Similar content being viewed by others


Abbreviations
- BPD:
-
biliopancreatic diversion
- GB:
-
gastric banding
- DS:
-
duodenal switch
- DVT:
-
deep venous thrombosis
- NMH:
-
heparin of low molecular weight
- PE:
-
pulmonary embolism
- RYGBP:
-
Roux-en-Y gastric bypass
- SG:
-
sleeve gastrectomy
- VTE:
-
venous thromboembolism
- VSD:
-
ventricle septum defect
References
Deitel M. Overweight and obesity worldwide now estimated to involve 1.7 billion people. Obes Surg. 2003;13:329–30.
James PT, Rigby N, Leach R. The obesity epidemic, metabolic syndrome and future prevention strategies. Eur J Cardiovasc Prev Rehabil. 2004;11:3–8.
Sjöström L, Narbro K, Sjöström CD, Karason K, Larsson B, Wedel H, et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357:741–52.
Hartel W, Euche A, Koppenhagen K et al. Leitlinien zur stationären und ambulanten Thrombembolie-Prophylaxe in der Chirurgie. Expertengespräche zur Thrombembolie-Prophylaxe 1997 und 2000. Beilage zu den Mitteilungen der Deutschen Gesellschaft für Chirurgie 2000;3.
Partsch H, Blättler W. Leitlinien zur Thrombembolie-Prophylaxe. Phlebologie. 2000;29:106–13.
International Consensus Statement. Prevention and treatment of venous thromboembolism. Int Angiol. 2006;25:101–61.
Clinical Issues Committee of the American Society for Metabolic and Bariatric Surgery. Prophylactic measures to reduce the risk of venous thromboembolism in bariatric surgery patients. Surg Obes Relat Dis. 2007;3:494–5.
Martin LF, Gouda BP. What we know and don’t know about deep venous thrombosis and pulmonary embolism!. Obes Surg. 2005;15:565–6. 1.
Stroh C, Birk D, Flade-Kuthe R, Frenken M, Herbig B, Höhne S, Köhler H, Lange V, Ludwig K, Matkowitz R, Meyer G, Meyer F, Pick P, Horbach T, Krause S, Schäfer L, Schlensak M, Shang E, Sonnenberg T, Susewind M, Voigt H, Weiner R, Wolff S, Lippert H, Wolf AM, Schmidt U, Manger T; Bariatric Surgery Working Group. A nationwide survey on bariatric surgery in Germany—results 2005–2007. Obes Surg. 2008 (in press).
Stroh C, Manger T. Studie zur Qualitätskontrolle der operativen Therapie der Adipositas. Mitt Dtsch Ges Chir. 2004;33:389–91.
Blaszyk H, Wollan PC, Witkiewicz AK, Bjornsson J. Death from pulmonary thromboembolism in severe obesity: lack of association with established genetic and clinical risk factors. Virchows Arch. 1999;434:529–32.
Eriksson S, Backman L, Ljungstrom K. The incidence of clinical postoperative thrombosis after gastric surgery for morbid obesity during 16 years. Obes Surg. 1997;7:332–6.
Hamad GG, Smith-Choban P. Enoxaparin for thromboprophylaxis in morbidly obese patients undergoing bariatric surgery: findings of the prophylaxis against VTE outcomes in bariatric surgery patients receiving Enoxaparin (PROBE) study. Obes Surg. 2005;15:1368–74.
Poulose BK, Griffin MR, Zhu Y, Smalley W, Richards WO, Wright JK, et al. National analysis of adverse patient safety for events in bariatric surgery. Am Surg. 2005;71:406–13.
Westling A, Bergquist D, Boström A, Karacagil S, Gustavsson S. Incidence of deep venous thrombosis in patients undergoing obesity surgery. World J Surg. 2002;26:470–3.
Fernandez A, DeMaria E, Tichansky D. Multivariate analysis of risk factors for death following gastric bypass for treatment of morbid obesity. Ann Surg. 2004;239:698–703.
DeMaria EJ, Portenier D, Wolfe L. Obesity surgery mortality risk score: proposal for a clinically useful score to predict mortality risk in patients undergoing gastric bypass. Surg Obes Relat Dis. 2007;3:134–40.
Melinek J, Livingston E, Cortina G, Fishbein MC. Autopsy findings following gastric bypass surgery for morbid obesity. Arch Pathol Lab Med. 2002;126:1091–5.
Nguyen NT, Owings JT, Gosselin R, Pevec WC, Lee SJ, Goldman C, et al. Systemic coagulation and fibrinolysis after laparoscopic and open gastric bypass. Arch Surg. 2001;136:909–16.
Miller MT, Rovito PF. An approach to venous thromboembolism prophylaxis in laparoscopic Roux-en-Y gastric bypass surgery. Obes Surg. 2004;14(6):731–7.
Sobolewski AP, Deshmukh RM, Brunson BL, McDevitt DT, VanWagenen TM, Lohr JM, et al. Venous hemodynamic changes during laparoscopic cholecystectomy. J Laparoendosc Surg. 1995;5:363–9.
Gargiulo NJ 3rd, Veith FJ, Lipsitz EC, Suggs WD, Ohki T, Goodman E, et al. The incidence of pulmonary embolism in open versus laparoscopic gastric bypass. Ann Vasc Surg. 2007;21:556–9.
Sugerman HJ, Sugerman EL, Wolfe L, Kellum JM Jr, Schweitzer MA, DeMaria EJ. Risks and benefits of gastric bypass in morbidly obese patients with severe venous stasis disease. Ann Surg. 2001;234:41–6.
Frezza EE, Wachtel MS. A simple venous thromboembolism prophylaxis protocol for patients undergoing bariatric surgery. Obesity (Silver Spring). 2006;14:1961–5.
Gargiulo NJ 3rd, Veith FJ, Lipsitz EC, Suggs WD, Ohki T, Goodman E. Experience with inferior vena cava filter placement in patients undergoing open gastric bypass procedures. J Vasc Surg. 2006;44:1301–5.
Prystowsky JB, Morasch MD, Eskandari MK, Hungness ES, Nagle AP. Prospective analysis of the incidence of deep venous thrombosis in bariatric surgery patients. Surgery. 2005;138:759–63. discussion 763-5.
Trigilio-Black CM, Ringley CD, McBride CL, Sorensen VJ, Thompson JS, Longo GM, et al. Inferior vena cava filter placement for pulmonary embolism risk reduction in super morbidly obese undergoing bariatric surgery. Surg Obes Relat Dis. 2007;3:461–4.
Obeid FN, Bowling WM, Fike JS, Durant JA. Efficacy of prophylactic inferior vena cava filter placement in bariatric surgery. Surg Obes Relat Dis. 2007;3:606–8. discussion 609-10.
Halmi D, Kolesnikov E. Preoperative placement of retrievable inferior vena cava filters in bariatric surgery. Surg Obes Relat Dis. 2007;3:602–5.
Wu EC, Barba CA. Current practices in the prophylaxis of venous thromboembolism in bariatric surgery. Obes Surg. 2000;10:7–13. discussion 14.
Gugliotti DV. What is the optimal venous thromboembolism prophylaxis for patients undergoing bariatric surgery? IMPACT consults. Proceedings of the 2nd Annual Cleveland Clinic Perioperative Medicine Summit. Cleve Clin J Med. 2006;73(Electronic Suppl 1):S17–8.
Scholten DJ, Hoedema RM, Scholten SE. A comparison of two different prophylactic dose regimens of low molecular weight heparin in bariatric surgery. Obes Surg. 2002;12:19–24.
Kalfarentzos F, Stavropoulou F, Yarmenitis S, Kehagias I, Karamesini M, Dimitrakopoulos A, et al. Prophylaxis of venous thromboembolism using two different doses of low-molecular-weight heparin (nadroparin) in bariatric surgery: a prospective randomized trial. Obes Surg. 2001;11:670–6.
Shuhaiber J, Vitello J. Is gastric bypass associated with more complications in patients weighing >500 lb (>227 kg)? Obes Surg. 2004;14:43–6.
Shepherd MF, Rosborough TK, Schwartz ML. Heparin thromboprophylaxis in gastric bypass surgery. Obes Surg. 2003;13:249–53.
Shepherd FM, Rosborough TK, Schwartz ML. Unfractionated heparin infusion for thromboprophylaxis in highest risk gastric bypass surgery. Obes Surg. 2004;14:601–5. 18.
Paige JT, Gouda BP, Gaitor-Stampley V, Scalia PG, Klainer TE, Raum WJ, et al. No correlation between anti-factor Xa levels, low-molecular-weight heparin, and bleeding after gastric bypass. Surg Obes Relat Dis. 2007;3:469–75.
Rocha AT, de Vasconcellos AG, da Luz Neto ER, Araújo DM, Alves ES, Lopes AA. Risk of venous thromboembolism and efficacy of thromboprophylaxis in hospitalized obese medical patients and in obese patients undergoing bariatric surgery. Obes Surg. 2006;16:1645–55.
Carmody BJ, Sugerman H, Kellum JM, Jamal MK, Johnson JM, Carbonell AM, et al. Pulmonary embolism complicating bariatric surgery: detailed analysis of a single institution’s 24-year experience. J Am Coll Surg. 2006;203:831–6.
Gonzalez R, Haines K, Nelson LG, Gallagher SF, Murr MM. Predictive factors of thromboembolic events in patients undergoing Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2006;2:30–5. discussion 35-6.
Sapala JA, Wood MH, Schuhknecht MP, Sapala MA. Fatal pulmonary embolism after bariatric operations for morbid obesity: a 24-year retrospective analysis. Obes Surg. 2003;13:819–25.
Mason EE, Renquist KE, Jiang D. Perioperative risks and safety of surgery for severe obesity. Am J Clin Nutr. 1992;55(2 Suppl):573S–6.
Holmes NJ, Brolin RE, Kaufman JL. Is morbid obesity a risk factor for postoperative venous thromboembolism? Complications in Surgery. 1996;13:23–8.
Husemann B, Reiners V. Initial outcome of vertical gastroplasty in treatment of morbid obesity. Zentralbl Chir. 1996;121:370–5.
Rutledge R. The mini-gastric bypass: experience with the first 1,274 cases. Obes Surg. 2001;11:276–80.
Semple CW, Chehata A, Wilkinson S, Wertheimer MA. Laparoscopic adjustable gastric banding: initial Tasmanian experience. ANZ J Surg. 2003;73(8):594–6.
Gonzalez QH, Tishler DS, Plata-Munoz JJ, Bondora A, Vickers SM, Leath T, et al. Incidence of clinically evident deep venous thrombosis after laparoscopic Roux-en-Y gastric bypass. Surg Endosc. 2004;18:1082–4.
Cotter SA, Cantrell W, Fisher B, Shopnick R. Efficacy of venous thromboembolism prophylaxis in morbidly obese patients undergoing gastric bypass surgery. Obes Surg. 2005;15:1316–20.
Quebbemann BB, Dallal RM. The orientation of the antecolic Roux limb markedly affects the incidence of internal hernias after laparoscopic gastric bypass. Obes Surg. 2005;15:766–70. discussion 770.
Heffline MS. Preventing vascular complications after gastric bypass. J Vasc Nurs. 2006;24:50–4. quiz 55.
Angstadt J, Whipple O. Developing a new bariatric surgery program. Am Surg. 2007;73:1092–7.
Cossu ML, Pilo L, Piseddu G, Tilocca PL, Cossu F, Noya G. Prophylaxis of venous thromboembolism in bariatric surgery. Chir Ital. 2007;59:331–5.
Nguyen NT, Hinojosa M, Fayad C, Varela E, Wilson SE. Use and outcomes of laparoscopic versus open gastric bypass at academic medical centers. J Am Coll Surg. 2007;205:248–55.
Kothari SN, Lambert PJ, Mathiason MA. Best Poster Award. A comparison of thromboembolic and bleeding events following laparoscopic gastric bypass in patients treated with prophylactic regimens of unfractionated heparin or enoxaparin. Am J Surg. 2007;194:709–11.
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
About this article
Cite this article
Stroh, C., Birk, D., Flade- Kuthe, R. et al. Evidence of Thromboembolism Prophylaxis in Bariatric Surgery—Results of a Quality Assurance Trial in Bariatric Surgery in Germany from 2005 to 2007 and Review of the Literature. OBES SURG 19, 928–936 (2009). https://doi.org/10.1007/s11695-009-9838-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-009-9838-2