
Abstract
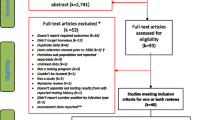
Despite its benefit for treating active tuberculosis, directly observed therapy (DOT) for latent tuberculosis infection (LTBI) has been largely understudied among challenging inner city populations. Utilizing questionnaire data from a comprehensive mobile healthcare clinic in New Haven, CT from 2003 to July 2011, a total of 2,523 completed tuberculin skin tests (TSTs) resulted in 356 new LTBIs. Multivariate logistic regression correlated covariates of the two outcomes (a) initiation of isoniazid preventative therapy (IPT) and (b) completion of 9 months of IPT. Of the 357 newly positive TSTs, 86.3 % (n = 308) completed screening chest radiographs (CXRs): 90.3 % (n = 278) were normal, and 0.3 % (n = 1) had active tuberculosis. Of those completing CXR screening, 44.0 % (n = 135) agreed to IPT: 69.6 % (n = 94) selected DOT, and 30.4 % (n = 41) selected self-administered therapy (SAT). Initiating IPT was correlated with undocumented status (AOR = 3.43; p < 0.001) and being born in a country of highest and third highest tuberculosis prevalence (AOR = 14.09; p = 0.017 and AOR = 2.25; p = 0.005, respectively). Those selecting DOT were more likely to be Hispanic (83.0 vs 53.7 %; p < 0.0001), undocumented (57.4 vs 41.5 %; p = 0.012), employed (p < 0.0001), uninsured (p = 0.014), and have stable housing (p = 0.002), no prior cocaine or crack use (p = 0.013) and no recent incarceration (p = 0.001). Completing 9 months of IPT was correlated with no recent incarceration (AOR 5.95; p = 0.036) and younger age (AOR 1.03; p = 0.031). SAT and DOT participants did not significantly differ for IPT duration (6.54 vs 5.68 months; p = 0.216) nor 9-month completion (59.8 vs 46.3 %; p = 0.155). In an urban mobile healthcare sample, screening completion for LTBI was high with nearly half initiating IPT. Undocumented, Hispanic immigrants from high prevalence tuberculosis countries were more likely to self-select DOT at the mobile outreach clinic, potentially because of more culturally, linguistically, and logistically accessible services and self-selection optimization phenomena. Within a diverse, urban environment, DOT and SAT IPT models for LTBI treatment resulted in similar outcomes, yet outcomes were hampered by differential measurement bias between DOT and SAT participants.


Similar content being viewed by others


References
World Health Organization. (2012). Global tuberculosis report 2012: Tuberculosis executive summary. Geneva: Switzerland.
Centers for Disease Control and Prevention. (2012). Trends in tuberculosis—United States, 2011. MMWR, 61(11), 181–189.
Jackman, S. (2000). Estimation and inference via Bayesian simulation: An introduction to Markov Chain Monte Carlo. American Journal of Political Science, 44, 375–404.
Hirsch-Moverman, Y., Bethel, J., Colson, P. W., Franks, J., & El-Sadr, W. (2010). Predictors of latent tuberculosis infection treatment completion in the United States: An inner city experience. The International Journal of Tuberculosis and Lung Disease, 14(9), 1104–1111.
Lazar, C., Sosa, L., & Lobato, M. (2008). Practices and policies of providers testing school-aged children for tuberculosis, Connecticut. Journal of Community Health, 2010(35), 495–499.
Guh, A., Sosa, L., Hadler, J. L., & Lobato, M. N. (2011). Missed opportunities to prevent tuberculosis in foreign-born persons, Connecticut, 2005–2008. The International Journal of Tuberculosis and Lung Disease, 15(8), 1044–1049.
Altice, F. L., Maru, D. S., Bruce, R. D., Springer, S. A., & Friedland, G. H. (2007). Superiority of directly administered antiretroviral therapy over self-administered therapy among HIV-infected drug users: A prospective, randomized, controlled trial. Clinical Infectious Diseases, 45(6), 770–778.
Macalino, G. E., Hogan, J. W., Mitty, J. A., Bazerman, L. B., Delong, A. K., Loewenthal, H., et al. (2007). A randomized clinical trial of community-based directly observed therapy as an adherence intervention for HAART among substance users. AIDS, 21(11), 1473–1477.
Berg, K. M., Litwin, A., Li, X., Heo, M., & Arnsten, J. H. (2011). Directly observed antiretroviral therapy improves adherence and viral load in drug users attending methadone maintenance clinics: A randomized controlled trial. Drug and Alcohol Dependence, 113(2–3), 192–199.
Bruce, R., Eiserman, J., Acosta, A., Gote, C., Lim, J., & Altice, F. (2012). Developing a modified directly observed therapy intervention for hepatitis C treatment in a methadone maintenance treatment program: Implications for program replication. American Journal of Drug and Alcohol Abuse, 38(3), 206–212.
Enders, C. (2010). Applied missing data analysis. New York: Guilford Press.
Liebman, J., Lamberti, P., & Altice, F. (2002). Effectiveness of a mobile medical van in providing screening services for STDs and HIV. Public Health Nursing, 19(5), 345–353.
Altice, F. L., Bruce, R. D., Walton, M. R., & Buitrago, M. I. (2005). Adherence to hepatitis B virus vaccination at syringe exchange sites. Journal of Urban Health, 82(1), 151–161.
Weiss, L., Netherland, J., Egan, J. E., Flanigan, T. P., Fiellin, D. A., Finkelstein, R., et al. (2011). Integration of buprenorphine/naloxone treatment into HIV clinical care: Lessons from the BHIVES collaborative. Journal of Acquired Immune Deficiency Syndromes, 56(S1), S68–S75.
Altice, F. L., Bruce, R. D., Lucas, G. M., Lum, P. J., Korthuis, P. T., Flanigan, T. P., et al. (2011). HIV treatment outcomes among HIV-infected, opioid-dependent patients receiving buprenorphine/naloxone treatment within HIV clinical care settings: Results from a multisite study. Journal of Acquired Immune Deficiency Syndromes, 56(S1), S22–S32.
Springer, S. A., Chen, S., & Altice, F. L. (2010). Improved HIV and substance abuse treatment outcomes for released HIV-infected prisoners: The impact of buprenorphine treatment. Journal of Urban Health, 87(4), 592–602.
Sullivan, L. E., Bruce, R. D., Altice, F. L., Haltiwanger, D., Lucas, G. M., Eldred, L., et al. (2006). Initial strategies for integrating buprenorphine into HIV care settings in the United States. Clinical Infectious Diseases, 43(S4), S191–S196.
Schwarz, R. K., Bruce, R. D., Ball, S. A., Herme, M., & Altice, F. L. (2009). Comparison of tuberculin skin testing reactivity in opioid-dependent patients seeking treatment with methadone versus buprenorphine: Policy implications for tuberculosis screening. American Journal of Drug and Alcohol Abuse, 35(6), 439–444.
Maru, D. S., Bruce, R. D., Walton, M., Springer, S. A., & Altice, F. L. (2009). Persistence of virological benefits following directly administered antiretroviral therapy among drug users: Results from a randomized controlled trial. Journal of Acquired Immune Deficiency Syndromes, 50(2), 176–181.
Maru, D. S., Bruce, R. D., Walton, M., Mezger, J. A., Springer, S. A., Shield, D., et al. (2008). Initiation, adherence, and retention in a randomized controlled trial of directly administered antiretroviral therapy. AIDS and Behavior, 12(2), 284–293.
Altice, F. L., Mezger, J. A., Hodges, J., Bruce, R. D., Marinovich, A., Walton, M., et al. (2004). Developing a directly administered antiretroviral therapy intervention for HIV-infected drug users: Implications for program replication. Clinical Infectious Diseases, 38(S5), S376–S387.
Smith-Rohrberg, D., Mezger, J., Walton, M., Bruce, R. D., & Altice, F. L. (2006). Impact of enhanced services on virologic outcomes in a directly administered antiretroviral therapy trial for HIV-infected drug users. Journal of Acquired Immune Deficiency Syndromes, 43(S1), S48–S53.
Saber-Tehrani A. S., Springer S. A., Qiu J., Herme M., Wickersham J., & Altice F. L. (2012). Rationale, study design and sample characteristics of a randomized controlled trial of directly administered antiretroviral therapy for HIV-infected prisoners transitioning to the community—a potential conduit to improved HIV treatment outcomes. Contemporary Clinical Trials, 33(2), 436–444.
World Health Organization. (2011). Guidelines for intensified tuberculosis case-finding and isoniazid preventative therapy for people living with HIV in resource-constrained settings. Geneva: Switzerland.
World Health Organization. (2011). Tuberculosis country profiles. http://www.who.int/tb/country/data/profiles/en/index.html. Accessed Nov 2012.
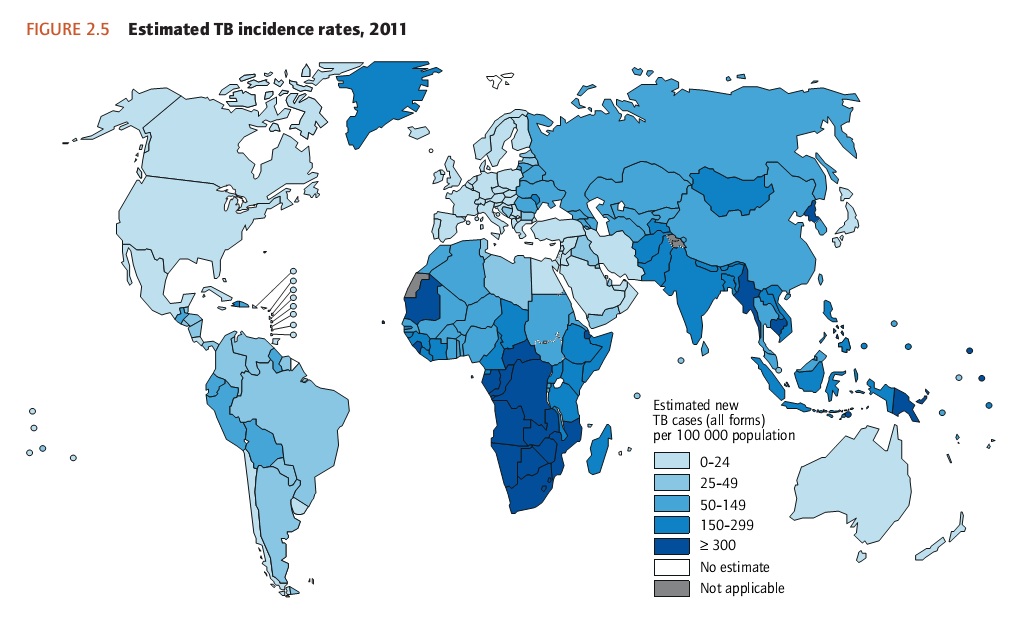
Stop TB Partnership. (2011). Global TB incidence rates. http://www.stoptb.org/assets/images/countries/map_incidence.jpg. Accessed Nov 2012.
StataCorp. (2011). Stata statistical software. College Station, TX: StataCorp LP.
Salomon, N., Perlman, D., Friedmann, P., Perkins, M. P., Ziluck, V., Des Jarlais, D., et al. (1999). Knowledge of tuberculosis among drug users relationship to return rates for tuberculosis screening at a syringe exchange. Journal of Substance Abuse Treatment, 16(3), 229–235.
Salomon, N., Perlman, D., Friedmann, P., Ziluck, V., & Des Jarlais, D. (2000). Prevalence and risk factors for positive tuberculin skin tests among active drug users at a syringe exchange program. The International Journal of Tuberculosis and Lung Disease, 4(1), 47–54.
Sterling, T. R., Villarino, M. E., Borisov, A. S., Shang, N., Gordin, F., Bliven-Sizemore, E., et al. (2011). Three months of rifapentine and isoniazid for latent tuberculosis infection. The New England Journal of Medicine, 365(23), 2155–2166.
{kind=link}
Acknowledgments
Angel Ojeda, Rolo Lopez, Lisandra Estremera, Elizabeth Roessler PA-C, Ruthanne Marcus, MPH, Natalie Lourenco, PA-C. Funding was provided by the National Institutes on Drug Abuse for Career Development (FLA: K24 DA017072; RDB: K23 DA022143) and Research (FLA: R01 DA13805, R01 DA017059, R01 DA029910), The National Institutes of Allergy and Infectious Diseases (JPM: T32 A1007517-12), and the Gilead Sciences Foundation.
Author information
Authors and Affiliations
Corresponding author
Additional information
Jamie P. Morano: This study was part of the Latent Tuberculosis Determinant and Treatment Adherence Project, LTBDATA.
Rights and permissions
About this article
Cite this article
Morano, J.P., Walton, M.R., Zelenev, A. et al. Latent Tuberculosis Infection: Screening and Treatment in an Urban Setting. J Community Health 38, 941–950 (2013). https://doi.org/10.1007/s10900-013-9704-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-013-9704-y