
Abstract
Objective
It is crucial to detect the unablated regions (=“gap”) in the radiofrequency linear ablation of atrial tachyarrhythmias. The purpose of this study was to examine the relationship between the electropysiological properties of the gap created in the canine atrium and its anatomicohistologic findings.
Methods and Results
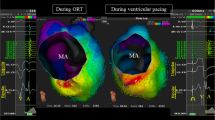
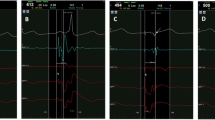
In 17 dogs, a linear epicardial radiofrequency ablation lesion was created on the right atrial wall with a gap of surviving tissue in the mid-portion of the lesion. For each gap, the local electrogram (LE) from the gap and conduction pattern through the gap were recorded using an electrode catheter and a plaque electrode during pacing from each side of the gap and the gap size was measured. The gaps >5 mm exhibited a conductive property and the gaps <3 mm had no conduction property according to 3-D mapping. The size of the conductive gaps was larger than that of the non-conductive gaps (7.1 ± 2.6 vs. 2.6 ± 2.5 mm, p < 0.0001). The LE configurations were categorized into single, double and continuous potentials and single potentials were demonstrated only in wide gaps >7 mm. There was a significant inversed correlation between the duration of the LE and gap size and also between the LE duration and the conduction velocity. Histological examination showed that the conduction properties through the gap depended mainly on its size.
Conclusions
The conductivity through the gap, which was affected by the size of the gap, may be evaluated by the duration and configuration of the local electrogram recorded from the gap.
Similar content being viewed by others

References
Tabuchi, T., Okumura, K., Matsunaga, T., Tsunoda, R., Jougasaki, M., & Yasue, H. (1995). Linear ablation of the isthmus between the Inferior Vena Cava and tricuspid annulus for the treatment of atrial flutter. Circulation, 92, 1312–1319.
Poty, H., Saouji, N., & Aziz, A. A. (1996). Radiofrequency catheter ablation of atrial flutter. Circulation, 94, 3204–3213.
Triedman, J. K., Saul, J. P., Weindling, S. N., & Walsh, E. P. (1995). Radiofrequency ablation of intra-atrial reentrant tachycardia after surgical palliation of congenital heart disease. Circulation, 91, 707–714.
Kalman, J. M., VanHare, G. F., Olgin, J. E., Saxon, L. A., Stark, S. I., & Lesh, M. D. (1996). Ablation of ‘Incisional’ reentrant atrial tachycardia complicating surgery for congenital heart disease. Circulation, 93, 502–512.
Anne, W., Rensburg, H. V., Adams, J., Ector, H., Vand de Werf, F., & Heidbuchel, H. (2002). Ablation of post-surgical intra-atrial reentrant tachycardia. Predilection target sites and mapping approach. European Heart Journal, 23, 1609–1616.
Shah, D., Haissaguerre, M., Jais, P., Fischer, B., Takahashi, A., Hocini, M., et al. (1997). Simplified electrophysiologically directed catheter ablation of recurrent common atrial flutter. Circulation, 96, 2505–2508.
Yamabe, H., Okumura, K., Misumi, I., Fukushima, H., Ueno, K., Kimura, Y., et al. (1999). Role of bipolar electrogram polarity mapping in localizing recurrent conduction in the isthmus early and late after ablation of atrial flutter. Journal of the American College of Cardiology, 33, 39–45.
Sra, J., Bhatia, A., Dhala, A., Blanck, Z., Rathod, S., Boveja, B., et al. (2000). Electroanatomic mapping to identify breakthrough sites in recurrent typical human flutter. Pacing and Clinical Electrophysiology, 23, 1479–1492.
Shah, D., Haissaguerre, M., Jais, P., Takahashi, A., Hocini, M., & Clementy, J. (1999). High density mapping of activation through an incomplete isthmus ablation line. Circulation, 99, 211–215.
Friedman, P. A., Luria, D., Munger, T. M., Jahangi, A., Shen, W. K., Rea, R. F., et al. (2002). Progressive isthmus delay during atrial flutter ablation; the critical importance of isthmus spanning electrodes for distinguishing pseudoblock from block. Pacing and Clinical Electrophysiology, 25, 308–315.
Chen, J., de Chillou, C., Hoff, P. I., Rossvoll, O., Andronasche, M., Sadoul, N., et al. (2002). Identification of extremely slow conduction in the cavotricuspid isthmus during common atrial flutter ablation. Journal of Interventional Cardiac Electrophysiology, 7, 67–75.
Tai, C. T., Haque, A., Lin, Y. K., Tsao, H. M., Ding, Y. A., Chang, M. S., et al. (2002). Double potential interval and transisthmus conduction time for prediction of cavotricuspid isthmus block after ablation of typical trial flutter. Journal of Interventional Cardiac Electrophysiology, 7, 77–82.
Perez, F. J., Wood, M. A., & Schubert, M. (2006). Effects of gap geometry on conduction through discontinuous radiofrequency lesions. Circulation, 113, 1723–1729.
Chorro, F. J., Mainar, L., Sanchis, J., Canoves, J., Llavador, E., Such, L. M., et al. (2001). Mapping of atrial activation patterns after inducing contiguous radiofrequency lesiongs: An experimental study. Pacing and Clinical Electrophysiology, 24, 147–156.
Thomas, S. P., Wallace, E. M., & Ross, D. L. (2001). The effect of a residual isthmus of surviving tissue on conduction after linear ablation in atrial myocardium. Journal of Interventional Cardiac Electrophysiology, 24, 147–156.
Tada, H., Oral, H., Sticherling, C., Chough, S. P., Baker, R. L., Wasmer, K., et al. (2001). Double potentials along the ablation line as a guide to radiofrequency ablation of typical trial flutter. Journal of the American College of Cardiology, 38, 750–755.
Inoue, H., & Zipes, D. P. (1987). Conduction over an isthmus of atrial myocardium in vivo: A possible model of Wolff–Parkinson–White syndrome. Circulation, 76, 637–647.
Mitchell, M. A., McRury, I. D., Everett, T. H., Li, H., Mangrum, J. M., & Haines, D. E. (1999). Morphological and physiological characteristics of discontinuous linear atrial ablations during atrial pacing and atrial fibrillation. Journal of Cardiovascular Electrophysiology, 10, 378–386.
Yamashita, T., Oikawa, N., Inoue, H., Murakawa, Y., Nakajima, T., Usui, M., et al. (1994). Slow abnormal conduction in the low right atrium: Its anatomic basis and relevance to atrial reentry. American Heart Journal, 127, 353–359.
Spach, M. S., Miller, W. T., Dolber, P. C., Kootsey, M., Sommer, J. R., & Mosher, C. E. (1982). The functional role of structural complexities in the propagation of depolarization in the atrium of the dog: Cardiac conduction disturbances due to discontinuities of effective axial resistivity. Circulation Research, 50, 175–191.
Cabo, C., Pertsov, A. M., Baxter, W. T., Davidenko, J. M., Gray, R. A., & Jalife, J. (1994). Wave-front curvature as a cause of slow conduction and block in isolated cardiac muscle. Circulation Research, 75, 1014–1028.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yano, K., Hirao, K., Horikawa, T. et al. Electrophysiology of a gap created on the canine atrium. J Interv Card Electrophysiol 17, 1–9 (2006). https://doi.org/10.1007/s10840-006-9059-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-006-9059-8