
Abstract
Background
The prone position during robotic esophageal mobilization for minimally invasive esophagectomy (MIE) provides several advantages with regards to operative times, surgeon ergonomics, and surgical view; however, this technique requires one-lung ventilation (OLV). There are no guidelines about ventilatory modes during OLV in the prone position. We investigated the effects of volume-controlled (VCV) and pressure-controlled ventilation (PCV) on oxygenation and intrapulmonary shunt during OLV in the prone position in patients who underwent robot-assisted esophagectomy.
Methods
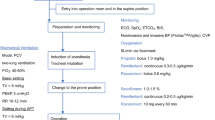
Eighteen patients, no major obstructive or restrictive pulmonary disease, were allocated randomly to one of two groups. In the first group (n = 9), OLV was started by VCV and the ventilator was switched to PCV after 30 minutes. In the second group (n = 9), the modes of ventilation were performed in the opposite order in the prone position. Hemodynamic and respiratory variables were obtained during OLV at the end of each ventilatory mode.
Results
There were no significant differences in arterial oxygen tension (PaO2), airway pressures, dynamic lung compliance, or physiologic dead space (Vd/Vt) during OLV between PCV and VCV in the prone position. Intrapulmonary shunt (Qs/Qt) was significantly lower with VCV than with PCV during OLV in the prone position (p = 0.044).
Conclusion
PCV provides no advantages compared with VCV with regard to respiratory and hemodynamic variables during OLV in the prone position. Either ventilatory mode can be safely used for patients who undergo robot-assisted esophagectomy and who have normal body mass index and preserved pulmonary function.
Similar content being viewed by others


References
Fabian T, Martin J, Katigbak M, McKelvey AA, Federico JA (2008) Thoracoscopic esophageal mobilization during minimally invasive esophagectomy: a head-to-head comparison of prone versus decubitus positions. Surg Endosc 22:2485–2491
Fabian T, McKelvey AA, Kent MS, Federico JA (2007) Prone thoracoscopic esophageal mobilization for minimally invasive esophagectomy. Surg Endosc 21:1667–1670
Palanivelu C, Prakash A, Senthilkumar R, Senthilnathan P, Parthasarathi R, Rajan PS, Venkatachlam S (2006) Minimally invasive esophagectomy: thoracoscopic mobilization of the esophagus and mediastinal lymphadenectomy in prone position–experience of 130 patients. J Am Coll Surg 203:7–16
Watanabe S, Noguchi E, Yamada S, Hamada N, Kano T (2000) Sequential changes of arterial oxygen tension in the supine position during one-lung ventilation. Anesth Analg 90:28–34
Ross DJ, Wu P, Mohsenifar Z (1997) Assessment of postural differences in regional pulmonary perfusion in man by single-photon emission computerized tomography. Clin Sci (Lond) 92:81–85
Pelosi P, Croci M, Calappi E, Cerisara M, Mulazzi D, Vicardi P, Gattinoni L (1995) The prone positioning during general anesthesia minimally affects respiratory mechanics while improving functional residual capacity and increasing oxygen tension. Anesth Analg 80:955–960
Manna EM, Ibraheim OA, Samarkandi AH, Alotaibi WM, Elwatidy SM (2005) The effect of prone position on respiratory mechanics during spinal surgery. Middle East J Anesthesiol 18:623–630
Tugrul M, Camci E, Karadeniz H, Sentürk M, Pembeci K, Akpir K (1997) Comparison of volume controlled with pressure controlled ventilation during one-lung anaesthesia. Br J Anaesth 79:306–310
Unzueta MC, Casas JI, Moral MV (2007) Pressure-controlled versus volume-controlled ventilation during one-lung ventilation for thoracic surgery. Anesth Analg 104:1029–1033
Heimberg C, Winterhalter M, Strüber M, Piepenbrock S, Bund M (2006) Pressure-controlled versus volume-controlled one-lung ventilation for MIDCAB. Thorac Cardiovasc Surg 54:516–520
Prella M, Feihl F, Domenighetti G (2002) Effects of short-term pressure controlled ventilation on gas exchange, airway pressures, and gas distribution in patients with acute lung injury/ARDS. Comparison with volume-controlled ventilation. Chest 122:1382–1388
Davis K Jr, Branson RD, Campbell RS, Porembka DT (1996) Comparison of volume control and pressure control ventilation: is flow waveform the difference? J Trauma 41:808–814
Maeda Y, Fujino Y, Uchiyama A, Matsuura N, Mashimo T, Nishimura M (2004) Effects of peak inspiratory flow on development of ventilator-induced lung injury in rabbits. Anesthesiology 101:722–728
Hardman JG, Aitkenhead AR (2003) Estimating alveolar dead space from the arterial to end-tidal CO2 gradient: a modeling analysis. Anesth Analg 97:1846–1851
Dharmavaram S, Jellish WS, Nockels RP, Shea J, Mehmood R, Ghanayem A, Kleinman B, Jacobs W (2006) Effect of prone positioning systems on hemodynamic and cardiac function during lumbar spine surgery: an echocardiographic study. Spine 31:1388–1394
Soro M, García-Pérez ML, Belda FJ, Ferrandis R, Aguilar G, Tusman G, Gramuntell F (2007) Effects of prone position on alveolar dead space and gas exchange during general anaesthesia in surgery of long duration. Eur J Anaesthesiol 24:431–437
Mentzelopoulos SD, Roussos C, Zakynthinos SG (2005) Prone position reduces lung stress and strain in severe acute respiratory distress syndrome. Eur Respir J 25:534–544
Albert RK, Hubmayr RD (2000) The prone position eliminates compression of the lungs by the heart. Am J Respir Crit Care Med 161:1660–1665
Mure M, Lindahl SG (2001) Prone position improves gas exchange—but how? Acta Anaesthesiol Scand 45:150–159
Mure M, Domino KB, Lindahl SGE, Hlastala MP, Altemeier WA, Glenny RW (2000) Regional ventilation-perfusion distribution is more uniform in the prone position. J Appl Physiol 88:1076–1083
Sentürk M (2006) New concepts of the management of one-lung ventilation. Curr Opin Anaesthesiol 19:1–4
Sentürk M (2007) Protective ventilation during one-lung ventilation. Anesthesiology 107:176–177
Stewart TE, Meade MO, Cook DJ, Granton JT, Hodder RV, Lapinsky SE, Mazer CD, McLean RF, Rogovein TS, Schouten BD, Todd TR, Slutsky AS (1998) Evaluation of a ventilation strategy to prevent Barotrauma in patients at high risk for acute respiratory distress syndrome. N Engl J Med 338:355–361
MacIntyre NR (1996) New modes of mechanical ventilation. Clin Chest Med 17:411–421
Cadi P, Guenoun T, Journois D, Chevallier JM, Diehl JL, Safran D (2008) Pressure-controlled ventilation improves oxygenation during laparoscopic obesity surgery compared with volume-controlled ventilation. Br J Anaesth 100:709–716
Campbell RS, Davis BR (2002) Pressure-controlled versus volume-controlled ventilation: does it matter? Respir Care 47:416–426
Esteban A, Alía I, Gordo F, de Pablo R, Suarez J, González G, Blanco J (2000) Prospective randomized trial comparing pressure-controlled ventilation and volume-controlled ventilation in ARDS. For the Spanish Lung Failure Collaborative Group. Chest 117:1690–1696
Edibam C, Rutten AJ, Collins DV, Bersten AD (2003) Effect of inspiratory flow pattern and inspiratory to expiratory ratio on nonlinear elastic behavior in patients with acute lung injury. Am J Respir Crit Care Med 167:702–707
Tusman G, Böhm SH, Vazquez de Anda GF, do Campo JL, Lachmann B (1999) ‘Alveolar recruitment strategy’ improves arterial oxygenation during general anaesthesia. Br J Anaesth 82:8–13
Mead J, Takishina T, Leith D (1970) Stress distribution in lungs: a model of pulmonary elasticity. J Appl Physiol 28:594–608
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Choi, Y.S., Shim, J.K., Na, S. et al. Pressure-controlled versus volume-controlled ventilation during one-lung ventilation in the prone position for robot-assisted esophagectomy. Surg Endosc 23, 2286–2291 (2009). https://doi.org/10.1007/s00464-008-0310-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-008-0310-5