
Abstract
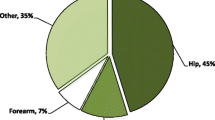
Osteoporosis can significantly impact on the risk of developing a fracture. Thus, fragility fractures represent a challenge for health professionals and decision makers of the twenty-first century. The aim of this work is to review the literature concerning osteoporotic fractures in Italy in terms of incidence, rate of hospitalization, relative risk of a new fragility fracture, and costs for the national health system. It was estimated that the costs of treating proximal femur fragility fractures in 2002 summed up to 1 billion Euros. The number of fragility fractures in Italy was calculated as follows: 91.494 hip fractures, 61.009 clinical vertebral fractures, 57.401 humeral fragility fractures, and 94.045 forearm/wrist fragility fractures. The incidence of fragility fractures in Italy is very high, and osteoporosis is the leading cause of morbidity in the Italian population.
Similar content being viewed by others

Introduction
Osteoporosis can significantly impact on the risk of developing a fracture. Thus, fragility fractures represent a challenge to health professionals and decision makers of the twenty-first century. The prevalence of osteoporosis in Italy was reported by the ESOPO study as follows: 23 % among all women, ranging from 9 % (40–49 years of age) to 45 % (>70 years of age), and almost 15 % in men aged over 60. The study estimated that about 4 million Italian women and 800,000 men were affected by osteoporosis [1]. As the population ages, the incidence of fragility fractures and chronic and degenerative diseases increases [2]. According to the World Health Organization (WHO), osteoporosis is a critical health problem second only to cardiovascular disease [3]. In Italy, the number of hospitalizations for hip fracture is comparable to that of acute myocardial infarction and the terms of management costs are even higher. For instance, Piscitelli et al. [4] estimated the cost of treating proximal femur fractures in 2002. The authors used diagnosis-related groups to calculate direct costs, reporting that a total of 1 billion Euros was disbursed in 2002. Specifically, 394 million Euros were spent on hospitalization costs, 412 million Euros for 1 month of rehabilitation, 108 million Euros for disability pensions, and 161 million Euros were indirect costs.
Vertebral fractures are the most common types of osteoporotic fractures: the EVOS study found that 12 % of men and women aged 50–80 years presented with radiographic evidence of vertebral deformities. About two-thirds of undiagnosed vertebral fractures present with back pain and physical impairment. Hence, the true incidence of these fractures may be significantly underestimated [5, 6]. Furthermore, increased risk of mortality and higher risk of subsequent fragility fractures are related to vertebral deformities [7, 8].
Hip fractures secondary to osteoporosis represent the most common fragility fractures requiring hospitalization and surgical treatment. The evidence in the literature strongly suggests that delayed surgical intervention affects outcome and increases the rate of general complications [9].
Wrist and forearm fractures are typical fractures affecting women in the peri-menopausal period, between the ages of 40 and 50 years. The female-to-male ratio is 4:1. The incidence of these fractures rapidly increases after menopause, and in men aged <70 years [10]. A wrist/forearm fracture is associated with a twofold increased risk of developing a vertebral or hip fracture, a 3.3 times higher risk of a new forearm fracture, and a 2.4 times higher risk of developing skeletal fractures elsewhere [11].
Fragility fractures of the humerus generally affect patients aged over 65 years. The humerus is the third most common fracture site in osteoporotic patients. Moreover, humeral fractures are associated with a fivefold increased risk of subsequent hip fracture in the following year [12].
“Minor” fragility fractures involve the foot, ankle, and ribs. As with other fragility fracture locations, the risk of developing a new osteoporotic fracture is doubled [11].
Tarantino et al. [13] reported on the incidence and hospitalization rate of fragility fractures in Italy based on a 3-year survey on 29.017 patients presenting to ten Emergency Departments. The authors observed 8.290 fragility hip fractures, 6.514 forearm/wrist fractures, 4.559 humeral fractures, 2.981 ankle fractures, and 2.927 vertebral fractures. The hospitalization rates were: 93.0 % for hip fractures, 22.6 % for forearm/wrist fractures, 36.3 % for humeral fractures, 31.3 % for ankle fractures, and 27.6 % for clinical vertebral fractures.
In their extension study, Piscitelli et al. [14] also estimated the number of fragility fractures in Italy subdivided by fracture site: 91.494 hip fractures, 61.009 clinical vertebral fractures, 57.401 humeral fragility fractures, and 94.045 forearm/wrist fragility fractures. Some differences in the number of estimated fractures are due to methodological choices.
Conclusion
The incidence of fragility fractures in Italy is very high, and osteoporosis is the leading cause of morbidity in the Italian population. All osteoporotic fractures should be considered as the first signal of an underlying disease. This condition represents a challenging problem for the national health system that requires effective prevention strategies.
References
Adami S, Giannini S, Giorgino R, Isaia G, Maggi S, Sinigaglia L, Filipponi P, Crepaldi G, Di Munno O (2003) The effect of age, weight, and lifestyle factors on calcaneal quantitative ultrasound: the ESOPO study. Osteoporos Int 14:198–207
Kanis JA, Burlet N, Cooper C, Delmas PD, Reginster JY, Borgstrom F, Rizzoli R (2008) European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO): European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 19:399–428
World Health Organization. WHO statistical information system (WHOSIS). [http://apps.who.int/ghodata/?vid=720]
Piscitelli P, Iolascon G, Gimigliano F, Muratore M, Camboa P, Borgia O, Forcina B, Fitto F, Robaud V, Termini G, Rini GB, Gianicolo E, Faino A, Rossini M, Adami S, Angeli A, Distante A, Gatto S, Gimigliano R, Guida G, SIOMMMS study group, CERSUM research group (2007) Incidence and costs of hip fractures compared to acute myocardial infarction in the Italian population: a 4 year survey. Osteoporos Int 18:211–219
O’Neill TW, Felsenberg D, Varlow J, Cooper C, Kanis JA, Silman AJ (1996) The prevalence of vertebral deformity in European men and women: the European Vertebral Osteoporosis Study. J Bone Miner Res 11:1010–1018
Nevitt MC, Ettinger B, Black DM et al (1998) The association of radiologically detected vertebral fracture with back pain and function: a prospective study. Ann Inter Med 128:793–800
Lindsay R, Silverman SL, Cooper C et al (2001) Risk of new vertebral fracture in the year following a fracture. JAMA 285:320–323
Ismail AA, O’neill TW, Cooper C et al (1998) Mortality associated with vertebral deformity in men and women: results from the European Prospective Osteoporosis Study (EPOS). Osteoporos Int 8:291–297
Rossini M, Piscitelli P, Fitto F, Camboa P, Angeli A, Guida G, Adami S (2005) Incidence and socioeconomic burden of hip fractures in Italy. Reumatismo 57(2):97–102
Cummings SR, Melton LJ (2002) Epidemiology and outcomes of osteoporotic fractures. Lancet 359(9319):1761–1767
Klotzbuecher CM, Ross PD, Landsmann PD, Abbott TA 3rd, Berger M (2000) Patients with prior fractures have an increased risk of future fractures: a summary of the literature and statistical synthesis. J Bone Miner Res 15(4):721–739
Clinton J (2009) Proximal humeral fracture as a risk factor for subsequent hip fractures. J Bone Jt Surg (American) 91:503–511
Tarantino U, Capone A, D’Arienzo M, Mauro GL, Impagliazzo A, Formica A, Pallotta F, Patella V, Spinarelli A, Pazzaglia U, Zarattini G, Roselli M, Montanari G, Sessa G, Privitera M, Verdoia C, Corradini C, Feola M, Padolino A, Saturnino L, Scialdoni A, Rao C, Iolascon G, Brandi ML, Piscitelli P (2010) The incidence of hip, forearm, humeral, ankle, and vertebral fragility fracture in Italy: results from a 3-year multi center study. Arthritis Res Ther 12:R226
Piscitelli P, Tarantino U, Chitano G, Argentiero A, Neglia C, Agnello N, Saturnino L, Feola M, Celi M, Raho C, Distante A, Brandi ML (2011) Updated incidence rates of fragility fractures in Italy: extension study 2002–2008. Clin Cases Miner Bone Metab 8(3):54–56
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ratti, C., Vulcano, E., La Barbera, G. et al. The incidence of fragility fractures in Italy. Aging Clin Exp Res 25 (Suppl 1), 13–14 (2013). https://doi.org/10.1007/s40520-013-0071-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-013-0071-4