
Abstract
This study aims to examine the needs and preferences regarding the delivery of health care services and information provision and their determinants in patients with systemic sclerosis (SSc). A questionnaire was sent to 77 SSc outpatients, comprising 27 items on health care needs within the domains physical, psychological, social support, employment/daily activities, or other health problems and 13 items on information needs. Moreover, the patients’ preferences regarding the provision of health care services and information were listed. Additional assessments included sociodemographic characteristics, physical functioning (SSc Health Assessment Questionnaire), and quality of life (SF-36). Sixty-four patients (83%) returned the questionnaire. Twenty-six patients (41%) reported one or more unmet health care needs, with the highest proportions of patients with unmet needs seen in the physical (28%) and psychological (20%) domain. The highest percentages of patients with information needs were observed for medical subjects (20–28%). A lower mental component summary scale score and younger age were associated with the presence of at least one health care need in the psychological domain. Worse physical functioning, a diagnosis of diffuse SSc and having a partner were associated with higher information need score. A yearly, standardized multidisciplinary assessment program was most frequently mentioned as a preferred, but not yet existing health care model (59%) and the rheumatologist as a preferred source of information supply (75%). Unmet health care and information needs are common among SSc patients. To improve SSc health care, more attention should be paid to health care services for specific physical and psychological problems and medical information supply by the rheumatologist. In addition, the development of new models of care, such as a yearly, standardized multidisciplinary diagnostic program seems warranted.
Similar content being viewed by others

Introduction
Systemic sclerosis (SSc) is a multisystem disease of unknown origin characterized by fibrosis of the skin and considerable morbidity [15]. Patients may suffer from dysfunction of lungs, kidneys, heart, gastrointestinal tract, and the musculoskeletal system, as well as digital ulcers, Raynaud’s phenomenon, and joint contractures. Two major subtypes are distinguished; diffuse cutaneous SSc (dcSSc) with skin thickening proximal to elbow and knees and limited cutaneous SSc (lcSSc) with involvement of the distal extremities. Given the complexity of the disease, SSc patients require multidisciplinary treatment by specialty physicians, health professionals such as physical therapists, occupational therapists, dieticians, and psychologists [3, 12, 18]. In recent years, SSc specific educational and rehabilitation programs have been developed [2, 7, 24].
Until now, little is known about how the available services relate to the health care needs of patients with SSc themselves. Rubenzik [23] found health care needs in the psychological/spiritual/existential domain in a group of 25 patients with SSc. In addition, in a Dutch study in 123 patients with SSc, the need for practical information on disease background, medication usage, and dealing with pain was identified [25]. However, in both studies it remained unclear to what extent the patients’ needs were met by current health care services delivery. Moreover, the association between needs and patient characteristics has only in part been studied [23]. None of these studies evaluated the patients’ preferences regarding the provision of their care, including their views on the institution of services that are not yet available.
The aim of this study was to identify unmet health care and information needs and their determinants as well as preferences for health care services delivery and information provision in patients with SSc.
Patients and methods
Study design
The study had a cross-sectional design. Ethical approval for this study was obtained from the Institutional Review Boards of the Leiden University Medical Center. All participants gave written informed consent.
Patients
Patients were recruited between May and July 2007. Inclusion criteria were: diagnosis of SSc as established by their treating rheumatologist according to ACR criteria [1], current treatment in the Leiden University Medical Center, being able to comprehend the Dutch questionnaire and age 18 years or older. A questionnaire was sent to all patients fulfilling these criteria, accompanied by an invitation letter, an information leaflet explaining the aim and the methods of the study, and a consent form. A follow-up letter was sent to participants who did not return the surveys within a month.
Assessment methods
Survey on health care and information needs and preferences.
-
(a)
Health care needs
Based on the Systemic Lupus Erythematosus Needs Questionnaire (SLENQ) [21], we developed a questionnaire including health problems relevant for patients with SSc within the following domains: physical (twelve items), psychological (nine items), social support (three items), and daily living/employment (three items). In addition to the 12 physical items, patients were invited to report ‘other physical issues’ in two text fields, in case these were not covered by the previous items. With every item, patients were asked to score the presence of a problem (no/sometimes/frequently/always; range 0–3). Per domain, the number of problems per patient was computed (score ranges physical domain 0–42, psychological domain 0–27, social domain, 0–9 and daily living employment domain 0–9). In addition, a total problem score was calculated (range 0–87).
If a problem was present, patients were then asked if they had discussed it with a health care provider (yes/no) and if not, whether there was an unmet need for contact with a health care provider regarding this problem (yes/no). A total score of unmet health care needs could be computed by adding up the number of unmet needs, ranging from 0 to 29.
The internal consistency of the questionnaire and its subscales was determined by computing Cronbach’s alpha for the health care problem score. In general, a Cronbach’s alpha of ≥0.70 is considered acceptable. For scales with a small number of items (social support and daily living/employment) and a low Cronbach’s alpha, a mean inter-item correlation was computed (optimal range recommended 0.2–0.4). Cronbach’s alpha of the total health care problem questionnaire was 0.90, whereas for the subscales Cronbach’s alpha was 0.79 for the physical domain, 0.89 for the psychological domain, 0.54 for the social support domain (inter-item correlation 0.34), and 0.78 for the daily living/employment domain.
As there is no gold standard for perceived health care needs, we determined the convergent validity of the questionnaire by examining the association between problem scores of the questionnaire and measures of physical and mental functioning. For this purpose, correlations were computed between the problem score of the physical domain on the one side and the Physical Component Summary Scale (PCSS) of the Short Form-36 (SF-36) and disability (HAQ score) on the other side and between the problem score of the psychological domain and the Mental Component Summary Scale of the SF-36 (MCSS; Pearson correlation coefficients). There were significant correlations between the physical symptoms score on the one side and the PCSS (r = −0.603, p < 0.01) and the HAQ (r = −0.598, p < 0.01) on the other side and between the psychological symptoms score and the MCSS (r = −0.740, p < 0.01).
-
(b)
Information needs
Again based on the SLENQ [21], 13 questions assessed the need for information on the following topics: Test results, medical treatment of SSc, knowing when to see a doctor, general information on medical tests, information on SSc, physical therapy, exercise and sports, the SSc patients society, occupational therapy, dental health, dietary information, counseling services, home (nursing) care. As compared to the SLENQ, the questions about physical activities and sports, physical therapy, and home (nursing) care were added. With every topic, the information need was scored on a five-point Likert scale: 1 = no need, 2 = low need, 3 = indifferent, 4 = moderate need, and 5 = high need. The scores were later dichotomized in two categories in the same manner as was done in the SLENQ: 0 ‘no need, low need or indifferent’ and 1 ‘moderate or high need’, so a total information need score could be computed, ranging from 0 to 13.
-
(c)
Preferences for health care delivery specifically for patients with SSc
Patients’ preferences regarding the delivery of health care in addition to regular outpatient clinic care included the following options: (1) multidisciplinary treatment if needed, (2) a yearly multidisciplinary diagnostic program with standardized measurement of disease activity and other medical assessments, (3) a yearly multidisciplinary diagnostic program with standardized measurement of disease activity and other medical assessments as well as an inventory of the patient’s personal need for health professionals’ care and information supply. Preferences were assessed on a five-point scale (1 = no need, 2 = low need, 3 = indifferent, 4 = moderate need, and 5 = high need).
-
(d)
Preferences regarding the provision of information
Patients were asked if they were to look for information in the next year, how they would rate their preferences for the following sources of information: internet, written information (leaflets), others coping with SSc, patient support group, information meeting in the hospital, group educational program (with or without family present), rheumatologist, general practitioner, or nurse specialist. Preference was evaluated by a five-point scale (1 = not at all preferred −5 = highly preferred).
An expert panel of three rheumatologists (AAS, GSB, JMvL) and a physician/epidemiologist (TVV) was responsible for the translation and adaptation of the SLENQ and the development of additional questions concerning preferences. Pilot testing by two SSc patients resulted in a few minor adjustments of the final questionnaire.
Socio-demographic characteristics
Socio-demographic variables included age (status of living (living with a partner yes/no), educational level: primary education (0–8 years, low education level), secondary education (9–16 years, medium education level), and higher vocational education/university (post-secondary, high education level) and paid employment (yes/no)).
Disease characteristics and function
Disease duration and disease subset (dcSSc or lcSSc) [15], were derived from the medical record. Disease onset was defined as time since diagnosis by the rheumatologist in either the Leiden University Medical Center (LUMC) or if applicable in another medical center (in years). In addition, patients were asked to fill in the SSc Health Assessment Questionnaire (SSc HAQ), a 20-item questionnaire comprising eight domains of activities of daily living, with the final score ranging from 0 (no disability) to 3 (severe disability) with scleroderma symptom visual analog scales (VAS 0–100 mm) in addition to Raynaud’s disease, digital ulcers, intestinal complaints, pulmonary complaints, overall complaints, and pain [4].The SSc HAQ has been found to be a reliable outcome measure for disease severity in SSc [20].
Quality of life
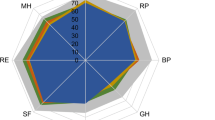
Quality of life was measured with the Short Form-36, which includes eight domain scores: physical functioning, role limitation due to physical problems, bodily pain, general health perception, vitality, social functioning, role limitation due to emotional problems, and mental health. The scores of the SF-36 subscales range from 0 to 100, with higher scores indicating better quality of life. The subscales can be converted into two summary scales: the physical and mental component summary scale, standardized to a score with a mean of 50 and a standard deviation of 10 in the general population. For that purpose, we used the scores from an age- and sex-matched, normative sample, drawn from a large, random, nationwide sample of adults (n = 1,742) from the general Dutch population Frequency Table and factor score coefficients [26]. The psychometric properties of this questionnaire have been found to be adequate [6].
Data analysis
Data entry was performed using Microsoft Office Access 2003. Statistical analyses were executed using SPSS 16.0 software.
Frequencies or means and standard deviations were calculated for each sociodemographic measure and disease characteristic, where appropriate. Comparisons of sociodemographic and disease characteristics of patients with limited and diffuse SSc were done with unpaired t tests, chi-square, or Fisher’s exact tests, where appropriate.
Descriptive statistics were employed for the patients’ needs and preferences regarding health care services and information delivery.
To determine which factors were associated with health care needs, logistic regression analysis was performed with socio-demographic and disease characteristics as independent variables and the health care need score, dichotomized into no need (0) and at least one need (≥1) as dependent variable. This analysis was repeated for each domain with the domain score dichotomized into no need (0) and at least one need (≥1) as dependent variable. To determine which factors were associated with information needs, linear regression analysis was performed, with socio-demographic and disease characteristics as independent variables and the information need score as dependent variable.
Results
Sociodemographics and disease characteristics
Of the patients, 48 of 77 responded to the initial mailing. After a reminder, another 16 returned the questionnaire, resulting in 64 responders (83%), four male and nine female non-responders. Socio-demographic and disease characteristics are presented in Table 1. In the lcSSc group, there were more females (p = 0.031) and patients with lcSSc had a significantly longer disease duration than patients with diffuse SSc (p = 0.019). There were no statistically significant differences in any other socio-demographic or disease characteristics between the two groups of patients.
Unmet health care needs
Table 2 presents the frequencies of reported health problems in the physical, psychological, social support and daily living/employment domains, contacts with physicians and/or health professional, and unmet health care needs regarding these issues. “Tiredness” (92%) and “Dealing with cold fingers” (91%) were problems that were most frequently mentioned. In total, 26 patients (41%) reported one or more unmet health care needs regarding the afore mentioned problems. The mean score for the physical problem scale was 17.2 (SD 8.1), psychological problem scale 6.7 (SD 5.3), daily living/employment problem scale 2.4 (SD 2.0), and social support 2.0 (SD 1.9), and total problem score 28.3 (SD 14.0).
The highest percentages of patients with an unmet need were seen within the physical domain (Table 2). The highest percentages of patients indicating at least one need was observed in the physical domain (28%), followed by the psychological (20%), social (14%), and daily living/employment (6%) domains.
Associations between sociodemographic and disease characteristics and health care needs
None of the socio-demographic and disease characteristics were significantly associated with a higher overall health care need (Table 3). Patients with at least one need in the physical domain were younger (50.3 (SD 16.1) versus 57.2 (11.5)), although the association was not significant (OR 0.96 (95%CI 0.92–1.0), p = 0.69). For the psychological domain, a lower mental component summary scale score (OR 0.92; 95%CI 0.87–0.99), p = 0.02 and younger age (OR 0.92; 95%CI 0.87–0.98), p = 0.01 were significantly associated with a higher health care need (results not shown).
Information needs
Table 4 shows the results of the patients’ needs regarding information. In the total group, the median total information need score was 6 (range 0–13). Fifty-five patients (86%) reported an information need regarding one or more of the 13 items. The topics showing the highest proportions of patients with a moderate or high information need included: test results (75%), medical tests you need (68%), medical treatment of SSc (59%), and knowing when to see a doctor (59%). A higher information need was significantly associated with dcSSc (adjusted for disease duration; beta 2.4, 95%CI 0.1–4.6, p = 0.039), a lower physical component summery scale SF-36 (beta 0.09, 95% CI 0.01–0.05, p = 0.048), and having a partner (beta 2.6, 95% CI 0.5–5.1, p = 0.046).
Preferences regarding specific health care services additional to regular outpatient clinic care
Table 5 shows the proportion of patients interested in specific forms of the delivery of multidisciplinary services specifically for patients with SSc. Overall, 45 of 64 (70%) patients had a moderate or high need for at least one of the comprehensive services specifically for SSc patients.
Preferences regarding the provision of information
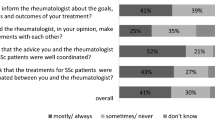
The rheumatologist was indicated as the preferred source of information in the nearby future by 75% of the patients (Table 6). Leaflets/books (63%), the Internet (61%), and group educational program in the hospital (58%) were more frequently indicated as a desired method of information delivery than information meetings organized by the Dutch Society of SSc patients, individual information provision by medical specialists other than the rheumatologist or by clinical nurse specialists (<50%).
Discussion
In this study on the needs of patients with SSc regarding the provision of health services and information, it was found that a number of patients indicated an unmet need for help regarding physical and/or mental problems. Information needs were most frequently mentioned with respect to medical issues. A substantial proportion of patients showed interest in various multidisciplinary services, and the rheumatologist was most often mentioned as the preferred provider of information.
Considering the impact of SSc on physical and psychosocial functioning and the usage of a high volume of physician services by SSc patients [3, 10], the lack of studies on patients’ needs, satisfaction, and preferences in health care is remarkable. In other rheumatic conditions, a high information need as well as a high percentage of unmet health care needs has been demonstrated [11, 14, 16].
In our study, the highest proportion of patients with at least one unmet need was seen in the physical domain. Our findings are difficult to compare directly with the published studies on unmet needs in SSc. Rubenzik [23] evaluated the needs of 25 SSc patients, nine diffuse, nine limited, and seven unsure subtype; but with the methodology employed in that study, questions based on a four-point scale (ranging from no need to high need), it remained unclear to what extent their indicated need for contact with a health professional was already satisfied. In patients with systemic lupus erythematosus [21], the physical domain had the highest proportion of participants with at least one unmet need. Rubenzik on the other hand, found high health care needs in nine out of ten items of the psychological/spiritual/existential domain and four out of 12 items in the physical domain, suggesting more needs in the psychological domain.
As compared to the needs of SLE patients [21] (where the number of patients with a need that was already satisfied were taken into account), our study demonstrate a relatively low percentage of patients with unmet needs. This may be because of the mild functional disability as demonstrated bij SF-36 and SSc HAQ outcomes in both the diffuse and limited cSSc group.
Concerning the association between disease characteristics and health care needs, worse mental functioning was significantly associated with the presence of at least one unmet need in the psychological domain. A previous study by Rubenzik did not examine the relationship of disease characteristics and health care needs, except for subtype. In 1,193 patients with rheumatoid arthritis and ankylosing spondylitis [14], unmet health care needs were likewise associated with worse health status. The lack of association between physical functioning and health care needs in our study may be explained by the relatively mild average level of functional disability. This may partly be due to the fact that 19 patients with diffuse systemic sclerosis had been effectively treated.
With respect to sociodemographic characteristics, in our study, a younger age was significantly associated with needs in the psychological domain. Rubenzik [23] found higher need in the social domain in patients with a rural background and a higher need in measures from the physical, psychological, daily living, and social domain in patients without a partner. In patients with rheumatoid arthritis and ankylosing spondylitis [14], no association of sex or age with health care needs was seen, whereas education was not evaluated.
Our study identified a considerable proportion of patients with a need for information, in particular on medical issues, including test results, medical treatment, and knowing when to see a doctor. These findings are in line with a Dutch study [25], where the need for information on various subjects was evaluated by a four-point Likert scale. Information on SSc (mean 2.29) had the highest score, followed by medication usage (1.77) and dealing with pain (1.77). In contrast, Rubenzik [23] concluded that there was not much need for medical information possibly because of the presumed increased publicly accessible information. Due to differences in study design, a direct comparison of the magnitude of the need for medical information between these studies is difficult. In recent years, publications on unmet information needs in other rheumatic diseases have demonstrated that patients have high desire for information [14, 19, 22]. Leung [16] found the highest unmet information need in psoriatic arthritis was advice on exercise (68%). Studies evaluating knowledge and information need of patients with rheumatoid arthritis (RA) mainly focused on the disease and on specialist medical care [5, 9, 17]. In general, these studies report a lack in of knowledge about the disease, medical care and medication. This is partly in line with our results.
We found that more information needs were associated with a subtype SSc as well as worse physical functioning and having a partner. The latter is surprising; discussing SSc-related problems with a partner may generate more information needs. Rubenzik [23] found more unmet needs in the domains health services, health information, and social support in patients with less education. In patients with RA, it was demonstrated the female gender [14] and lower age [8] were predictive for the presence of information needs. A significant difference in need for information between men and women, or lower and higher education was not observed in our results.
The preferences of SSc patients regarding the provision of SSc-specific health care programs and information have never been evaluated previously. Important findings are the preference of patients for their rheumatologist as source of information supply over any other type of information gathering, and the patients’ interest in a yearly daycare program with standardized assessment of the disease course in addition to regular outpatient clinic care. These findings are in line with results among patients with psoriatic arthritis, showing that a large proportion of patients are motivated to participate in various additional care programs [16].
Our study has a number of limitations. First, the study group is relatively small, although the number of participants is greater than the 25 patients studied in a previously published paper on unmet needs in systemic sclerosis [23]. Also, the cohort has relatively long disease duration, this is especially the case for the patients with dcSSc (average 6.4 years, SD 4.7). Therefore, the group of patients could probably be considered a survival cohort, which could explain the relatively mild level of functional disability as compared to other cohorts of patients with SSc [10, 13]. This selection bias could hamper the generalization of our data to patients with shorter disease duration and/or more active disease. As correlations between disease activity and stage and unmet needs may be identified by a larger study group cohort, further research is warranted.
Comparison with other patients groups may further be hampered by differences in healthcare systems and socio-economic background of patients.
Second, the questionnaire we used was based on the SLENQ, but was not yet validated in Dutch. Unfortunately, data collection was established prior to publication of the study by Rubenzik, who employed the Scleroderma Unmet Needs Index (SUNI), which was also based on the SLENQ. The items included in our questionnaire and the SUNI are largely comparable, but not identical. Finally, selection bias cannot be fully excluded since the response rate was 83%. On the other hand, a response rate of 83% is relatively high, and might probably express patients’ willingness to be engaged in the optimization of health care services.
In daily practice, our results imply that SSc patients may face several physical or psychological problems that are, according to a considerable number of patients, not sufficiently addressed by rheumatologists. These include physical symptoms as pain and or Raynaud’s phenomenon. The concurring need for guidance with respect to psychological issues, e.g., the uncertainty and fears patients that have to deal with, substantiates the need for a multidisciplinary approach. In our study, it was indeed demonstrated that a substantial proportion of patients showed interest in various multidisciplinary services. Another important finding in this study is the high information need in SSc patients, and the preference of the rheumatologist as information supplier. This suggests that health care in SSc should also focus on patient education. In outpatient clinic care, a rheumatologist can pay more attention to information supply. At the same time, patient education programs, involving a rheumatologist, may further improve the quality of SSc patient care.
References
Preliminary criteria for the classification of systemic sclerosis (scleroderma). Subcommittee for Scleroderma (1980) Criteria of the American Rheumatism Association Diagnostic and Therapeutic Criteria Committee: Arthritis Rheum 23:581–590
Antonioli CM, Bua G, Frige A, Prandini K, Radici S, Scarsi M, Danieli E, Malvicini A, Airo P (2009) An individualized rehabilitation program in patients with systemic sclerosis may improve quality of life and hand mobility. Clin Rheumatol 28:159–165
Bernatsky S, Panopolis P, Hudson M, Pope J, Leclercq S, Robinson D, Jones N, Markland J, bu-Hakima M, Mathieu JP, Docherty P, Khalidi N, Sutton E, Baron M (2009) Demographic and clinical factors associated with physician service use in systemic sclerosis. J Rheumatol 36:96–98
Clements PJ, Wong WK, Hurwitz EL, Furst DE, Mayes M, White B, Wigley F, Weisman M, Barr W, Moreland L, Medsger TA Jr, Steen V, Martin RW, Collier D, Weinstein A, Lally E, Varga J, Weiner SR, Andrews B, Abeles M, Seibold JR (2001) The Disability Index of the Health Assessment Questionnaire is a predictor and correlate of outcome in the high-dose versus low-dose penicillamine in systemic sclerosis trial. Arthritis Rheum 44:653–661
Edworthy SM, Devins GM, Watson MM (1995) The Arthritis Knowledge Questionnaire. A test for measuring patient knowledge of arthritis and its self-management. Arthritis Rheum 38:590–600
Essink-Bot ML, Krabbe PF, Bonsel GJ, Aaronson NK (1997) An empirical comparison of four generic health status measures. The Nottingham Health Profile, the Medical Outcomes study 36-item Short-Form Health Survey, the COOP/WONCA Charts, and the EuroQol Instrument. Med Care 35:522–537
Genth E, Baltscheit C (2003) Patient education “systemic sclerosis”. Z Rheumatol 62:II24–II25
Gordon MM, Capell HA, Madhok R (2002) The use of the Internet as a resource for health information among patients attending a rheumatology clinic. Rheumatology (Oxford) 41:1402–1405
Hennell SL, Brownsell C, Dawson JK (2004) Development, validation and use of a Patient Knowledge Questionnaire (PKQ) for patients with early rheumatoid arthritis. Rheumatology (Oxford) 43:467–471
Hudson M, Thombs BD, Steele R, Panopalis P, Newton E, Baron M (2009) Quality of life in patients with systemic sclerosis compared to the general population and patients with other chronic conditions. J Rheumatol 36:768–772
Jacobi CE, Rupp I, Boshuizen HC, Triemstra M, Dinant HJ, van den Bos GA (2004) Unmet demands for health care among patients with rheumatoid arthritis: indications for underuse? Arthritis Rheum 51:440–446
Johnson SR, Carette S, Dunne JV (2006) Scleroderma: health services utilization from patients’ perspective. J Rheumatol 33:1123–1127
Khanna D, Ahmed M, Furst DE, Ginsburg SS, Park GS, Hornung R, Tsevat J (2007) Health values of patients with systemic sclerosis. Arthritis Rheum 57:86–93
Kjeken I, Dagfinrud H, Mowinckel P, Uhlig T, Kvien TK, Finset A (2006) Rheumatology care: involvement in medical decisions, received information, satisfaction with care, and unmet health care needs in patients with rheumatoid arthritis and ankylosing spondylitis. Arthritis Rheum 55:394–401
LeRoy EC, Black C, Fleischmajer R, Jablonska S, Krieg T, Medsger TA Jr, Rowell N, Wollheim F (1988) Scleroderma (systemic sclerosis): classification, subsets and pathogenesis. J Rheumatol 15:202–205
Leung YY, Tam LS, Lee KW, Leung MH, Kun EW, Li EK (2009) Involvement, satisfaction and unmet health care needs in patients with psoriatic arthritis. Rheumatology (Oxford) 48:53–56
Lineker SC, Badley EM, Hughes EA, Bell MJ (1997) Development of an instrument to measure knowledge in individuals with rheumatoid arthritis: the ACREU rheumatoid arthritis knowledge questionnaire. J Rheumatol 24:647–653
Mawdsley AH (2006) Patient perception of UK scleroderma services—results of an anonymous questionnaire. Rheumatology (Oxford) 45:1573
Meesters JJ, Vliet Vlieland TP, Hill J, Ndosi ME (2009) Measuring educational needs among patients with rheumatoid arthritis using the Dutch version of the Educational Needs Assessment Tool (DENAT). Clin Rheumatol 28:1073–1077
Merkel PA, Herlyn K, Martin RW, Anderson JJ, Mayes MD, Bell P, Korn JH, Simms RW, Csuka ME, Medsger TA Jr, Rothfield NF, Ellman MH, Collier DH, Weinstein A, Furst DE, Jimenez SA, White B, Seibold JR, Wigley FM (2002) Measuring disease activity and functional status in patients with scleroderma and Raynaud’s phenomenon. Arthritis Rheum 46:2410–2420
Moses N, Wiggers J, Nicholas C, Cockburn J (2005) Prevalence and correlates of perceived unmet needs of people with systemic lupus erythematosus. Patient Educ Couns 57:30–38
Neame R, Hammond A, Deighton C (2005) Need for information and for involvement in decision making among patients with rheumatoid arthritis: a questionnaire survey. Arthritis Rheum 53:249–255
Rubenzik TT, Derk CT (2009) Unmet patient needs in systemic sclerosis. J Clin Rheumatol 15:106–110
Samuelson UK, Ahlmen EM (2000) Development and evaluation of a patient education program for persons with systemic sclerosis (scleroderma). Arthritis Care Res 13:141–148
Teunissen, HA, van Lankveld WGJM, Vonk MC, van den Hoogen FHJ (2005) Systemische sclerose: de gevolgen voor het psychisch en lichamelijk functioneren, en de behoefte aan begeleiding. Nederlands tijdschrift voor reumatologie 2005(4), 33–39
Ware JE KMKS (1994) SF-36 Health Survey Manual and Interpretation Guide.
Acknowledgments
We would like to thank the patients with systemic sclerosis for their cooperation.
Disclosures
None
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Schouffoer, A.A., Zirkzee, E.J.M., Henquet, S.M. et al. Needs and preferences regarding health care delivery as perceived by patients with systemic sclerosis. Clin Rheumatol 30, 815–824 (2011). https://doi.org/10.1007/s10067-010-1645-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-010-1645-6