
Abstract
Background
In recent years, minilaparoscopic cholecystectomy (MLC; total size of trocar incision <25 mm) has been increasingly advocated for the removal of the gallbladder, due to potentially better surgical outcomes (e.g., better cosmetic result, reduced pain, shorter hospital stay, quicker return to activity), but an evidence-based approach has been lacking. The current systematic review was undertaken to evaluate the importance of total size of trocar incision in improving surgical outcomes in adult laparoscopic cholecystectomy (LC).
Methods
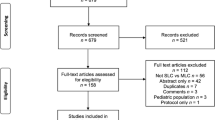
The literature was systematically reviewed using MEDLINE and EmBASE. Only randomized controlled trials in English, investigating minilaparoscopic versus conventional LC (total size of trocar incision ≥25 mm) and reporting pain scores were included. Quantitative analyses (meta-analyses) were performed on postoperative pain scores and other patient outcomes from more than one study where feasible and appropriate. Qualitative analyses consisted of assessing the number of studies showing a significant difference between the techniques.
Results
Thirteen trials met the inclusion criteria. There was a trend towards reduced pain with MLC compared with conventional LC, without reduction in opioid use. Patients in the MLC group had slightly reduced length of hospital stay, but there were no significant differences for return to activity. The two interventions were also similar in terms of operating times and adverse events, but MLC was associated with better cosmetic result (largely patient rated). There was a significantly greater likelihood of conversion to conventional LC or to open cholecystectomy in the MLC group than there was of conversion to open cholecystectomy in the conventional LC group [OR 4.71 (95% confidence interval 2.67–8.31), p < 0.00001].
Conclusions
The data included in this review suggest that reducing the size of trocar incision results in some limited improvements in surgical outcomes after LC. However, it carries a higher risk of conversion to conventional LC or open cholecystectomy.




Similar content being viewed by others


References
Novitsky YW, Kercher KW, Czerniach DR, Kaban GK, Khera S, Gallagher-Dorval KA, Callery MP, Litwin DE, Kelly JJ (2005) Advantages of mini-laparoscopic vs conventional laparoscopic cholecystectomy: results of a prospective randomized trial. Arch Surg 140:1178–1183
Gupta A, Shrivastava UK, Kumar P, Burman D (2005) Minilaparoscopic versus laparoscopic cholecystectomy: a randomised controlled trial. Trop Gastroenterol 26:149–151
Bisgaard T, Klarskov B, Rosenberg J, Kehlet H (2001) Characteristics and prediction of early pain after laparoscopic cholecystectomy. Pain 90:261–269
Yuan RH, Lee WJ, Yu SC (1997) Mini-laparoscopic cholecystectomy: a cosmetically better, almost scarless procedure. J Laparoendosc Adv Surg Tech A 7:205–211
Kimura T, Sakuramachi S, Yoshida M, Kobayashi T, Takeuchi Y (1998) Laparoscopic cholecystectomy using fine-caliber instruments. Surg Endosc 12:283–286
Ngoi SS, Goh P, Kok K, Kum CK, Cheah WK (1999) Needlescopic or minisite cholecystectomy. Surg Endosc 13:303–305
Reardon PR, Kamelgard JI, Applebaum BA, Brunicardi FC (1999) Mini-laparoscopic cholecystectomy: validating a new approach. J Laparoendosc Adv Surg Tech A 9:227–232 discussion 232–233
Unger SW, Paramo JC, Perez M (2000) Microlaparoscopic cholecystectomy. Less invasive gallbladder surgery. Surg Endosc 14:336–339
Fischer HB, Simanski CJ (2005) A procedure-specific systematic review and consensus recommendations for analgesia after total hip replacement. Anaesthesia 60:1189–1202
Kehlet H, Wilkinson RC, Fischer HB, Camu F; on behalf of the PROSPECT Working Group (2007) PROSPECT: evidence-based, procedure-specific postoperative pain management. Best Pract Res Clin Anaesthesiol 21:149–159
Neugebauer EA, Wilkinson RC, Kehlet H, Schug SA; on behalf of the PROSPECT Working Group (2007) PROSPECT: a practical method for formulating evidence-based expert recommendations for the management of postoperative pain. Surg Endosc 21:1047–1053
Jadad AR, Moore A, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay H (1996) Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 17:1–12
Moher D, Schulz KF, Altman D; CONSORT Group (2005) The CONSORT Statement: revised recommendations for improving the quality of reports of parallel-group randomized trials 2001. Explore (NY) 1:40–45
The Cochrane Collaboration (2003) RevMan Analyses [Computer program]. Version 1.0 for Windows. In: Review Manager (RevMan) 4.2. Oxford, England
Ainslie WG, Catton JA, Davides D, Dexter S, Gibson J, Larvin M, McMahon MJ, Moore M, Smith S, Vezakis A (2003) Micropuncture cholecystectomy vs conventional laparoscopic cholecystectomy: a randomized controlled trial. Surg Endosc 175:766–772
Alponat A, Cubukcu A, Gonullu N, Canturk Z, Ozbay O (2002) Is minisite cholecystectomy less traumatic? Prospective randomized study comparing minisite and conventional laparoscopic cholecystectomies. World J Surg 2612:1437–1440
Bisgaard T, Klarskov B, Trap R, Kehlet H, Rosenberg J (2000) Pain after microlaparoscopic cholecystectomy. A randomized double-blind controlled study. Surg Endosc 14:340–344
Bisgaard T, Klarskov B, Trap R, Kehlet H, Rosenberg J (2002) Microlaparoscopic vs conventional laparoscopic cholecystectomy: a prospective randomized double-blind trial. Surg Endosc 16:458–464
Bresadola F, Pasqualucci A, Donini A, Chiarandini P, Anania G, Terrosu G, Sistu MA, Pasetto A (1999) Elective transumbilical compared with standard laparoscopic cholecystectomy. Eur J Surg 165:29–34
Cheah WK, Lenzi JE, So JB, Kum CK, Goh PM (2001) Randomized trial of needlescopic versus laparoscopic cholecystectomy. Br J Surg 88:45–47
Huang MT, Wang W, Wei PL, Chen RJ, Lee WJ (2003) Minilaparoscopic and laparoscopic cholecystectomy: a comparative study. Arch Surg 138:1017–1023
Leggett PL, Churchman-Winn R, Miller G (2000) Minimizing ports to improve laparoscopic cholecystectomy. Surg Endosc 14:32–36
Look M, Chew SP, Tan YC, Liew SE, Cheong DM, Tan JC, Wee SB, Teh CH, Low CH (2001) Post-operative pain in needlescopic versus conventional laparoscopic cholecystectomy: a prospective randomised trial. J R Coll Surg Edinb 463:138–142
Poon CM, Chan KW, Lee DW, Chan KC, Ko CW, Cheung HY, Lee KW (2003) Two-port versus four-port laparoscopic cholecystectomy. Surg Endosc 17:1624–1627
Sarli L, Iusco D, Gobbi S, Porrini C, Ferro M, Roncoroni L (2003) Randomized clinical trial of laparoscopic cholecystectomy performed with mini-instruments. Br J Surg 90:1345–1348
Schwenk W, Neudecker J, Mall J, Bohm B, Muller JM (2000) Prospective randomized blinded trial of pulmonary function, pain, and cosmetic results after laparoscopic vs microlaparoscopic cholecystectomy. Surg Endosc 14:345–348
Trichak S (2003) Three-port vs standard four-port laparoscopic cholecystectomy. Surg Endosc 17:1434–1436
Singh P, Kaushik R, Sharma R (2006) Umbilical port hernia following laparoscopic cholecystectomy. J Min Access Surg 2:29–30
Lau H, Lo CY, Patil NG, Yuen WK (2006) Early versus delayed-interval laparoscopic cholecystectomy for acute cholecystitis: a metaanalysis. Surg Endosc 20:82–87
Berci G (1998) Laparoscopic cholecystectomy using fine-caliber instruments. Smaller is not necessarily better. Surg Endosc 12:197
Acknowledgements
The authors would like to thank Caroline Sharp (M.Sci, Medical Writer, Choice Pharma, Hitchin, UK) for her help with data extraction and entry; Emmanuel Marret (M.D., Departement d’Anesthesie-Reanimation, Hôpital Tenon, Paris, France) for his expert statistical input; Iradj Reza (Ph.D., Biomedical Information Scientist, Pfizer, Sandwich, UK) for his help and expertise in performing literature searches in EmBASE and MEDLINE; and Roseanne Wilkinson (Ph.D., Senior Medical Writer, Choice Pharma), Christine Drewienkiewicz (B.Sc., Scientific Services Director, Choice Pharma), Eva Leung (B.Sc., Account Executive, Choice Pharma), and James Pickford (B.Sc., Editorial Director, Choice Pharma) for editorial assistance.
Financial support: All authors are members or associates of the PROSPECT working group, which is supported by Pfizer Inc., New York, NY, USA. The PROSPECT working group members have been reimbursed by Pfizer Inc. for attending PROSPECT meetings to formulate the consensus recommendations. D.R. is employed by Choice Pharma, which has received funding from Pfizer Inc. to implement PROSPECT activities. This paper makes no specific recommendations about the use of any medical products, drugs or equipment manufactured by Pfizer Inc. or by any of its subsidiaries.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
McCloy, R., Randall, D., Schug, S.A. et al. Is smaller necessarily better? A systematic review comparing the effects of minilaparoscopic and conventional laparoscopic cholecystectomy on patient outcomes. Surg Endosc 22, 2541–2553 (2008). https://doi.org/10.1007/s00464-008-0055-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-008-0055-1