
Abstract
Purpose
To determine, in a subset of children previously reported, if the time of day when adenotonsillectomy for severe obstructive sleep apnea syndrome (OSAS) was performed affected the incidence of postoperative respiratory complications.
Clinical features
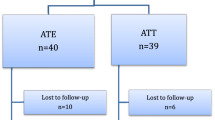
Children having adenotonsillectomy were included if they had a polysomnographic diagnosis of severe OSAS within six months prior to operation. Patients who met the inclusion criteria were grouped by the occurrence of postoperative desaturation into a saturated (SAT) and desaturated (deSAT) group. The charts of children in group deSAT were reviewed. The clock time of the surgical procedure was recorded and categorized as morning (AM) or afternoon (PM).
Results
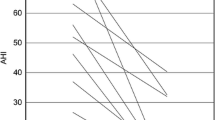
Eighty-eight patients met the inclusion criteria. There were 31 girls and 57 boys. The mean ± SD age (yr) and weight (kg) were 4.6 ± 2.9 yr and 20.8 ± 14.5 kg respectively. There were 63 children in the SATgroup and 25 in the deSATgroup. Differences in age, weight and gender were not significant. The preoperative oxygen saturation (SaO2) nadir for the SAT and deSAT groups was 80.8 ± 10.2% and 67.6 ± 17.5% (P < 0.05) respectively. The preoperative obstructive apnea and hypopnea index was 15.8 ± 10.2 and 35.7 ± 34.6 events · hr−1 (P < 0.05), respectively. Surgery in 63 (71.6%) children was performed in the AM. Univariate logistic regression identified PM surgery [odds ratio (OR) 4.6, 95% confidence interval (CI) 1.7 to 12.6,P = 0.002] and a preoperative SaO2 nadir < 80% (OR 3.6, 95% CI 1.4 to 9.4,P = 0.009) as risk factors predicting postadenotonsillectomy desaturation.
Conclusion
Children with severe OSAS whose surgery is performed in the AM are less likely to desaturate following adenotonsillectomy than children whose surgery is performed in the PM.
Résumé
Objectif
Déterminer, chez un sous-groupe connu d’enfants, si i’heure à iaqueiie i’amygdaiectomie a été réalisée pour un syndrome sévère d’apnée obstructive du sommeil (SAOS) a un effet sur l’incidence de complications respiratoires postopératoires.
Éléments cliniques
Des enfants subissant une amygdalectomie ont été inclus dans notre étude si un diagnostic polysomnographique de SAOS sévère avait été établi dans les six mois avant l’opération. Les patients admis ont été répartis selon l’occurrence de désaturation postopératoire dans un groupe de saturation (SAT) ou de désaturation (deSAT). Les dossiers des enfants du groupe deSAT ont été révisés. L’heure de l’opération a été notée sous matin (AM) ou après-midi (PM).
Résultats
Ont été admis à l’étude, 88 patients dont 31 files et 57 garçons. La moyenne d’âge et de poids ± l’écart type étaient respectivementde 4,6 ± 2,9 ans et 20,8 ± 14,5 kg. Il y a eu 63 enfants dans le groupe SAT et 25 dans le groupe deSAT. Les différences d’âge, de poids et de sexe n’étaient pas signifcatives. Le niveau préopératoire minimal de saturation en oxygène (SaO2) a été de 80,8 ± 10,2 % et de 67,6 ± 17,5 % (P < 0,05) dans les groupes SAT et deSAT respectivement. Les indices d’apnée obstructive et d’hypopnée préopératoires étaient de 15,8 ± 10,2 et de 35,7 ± 34,6 événements · h−1 (P < 0,05), respectivement. L’opération de 63 (71,6 %) enfants s’est faite en AM. Une analyse univariée de régression logistique a considéré l’opération réalisée en PM [risque relatif (RR) de 4,6, intervalle de confiance (IC) de 95 %, 1,7 à 12,6, P = 0,002] et un niveau minimal de SaO2 préopératoire < 80 % (RR de 3,6, IC de 95 %, 1,4 à 9,4, P = 0,009) comme des facteurs de risque prédictifs de désaturation postamygdalectomie.
Conclusion
Les enfants atteints d’un SAOS sévère, opérés en AM, sont moins susceptibles de subir une désaturation postamygdalectomie que les enfants opérés en PM.
Article PDF
Similar content being viewed by others

References
Rosenfeld RM, Green RP. Tonsillectomy and adenoidectomy: changing trends. Ann Otol Rhinol Laryngol 1990; 99: 187–91.
Pickering AE, Bridge HS, Nolan J, Stoddart PA. Double-blind, placebo-controlled analgesic study of ibuprofen or rofecoxib in combination with paracetamol for tonsillectomy in children. Br J Anaesth 2002; 88: 72–7.
Rosen GM, Muckle RP, Mahowald MW, Goding GS, Ullevig C. Postoperative respiratory compromise in children with obstructive sleep apnea syndrome: can it be anticipated? Pediatrics 1994; 93: 784–8.
McColley SA, April MM, Carroll JL, Naclerio RM, Loughlin GM. Respiratory compromise after adenotonsillectomy in children with obstructive sleep apnea. Arch Otolaryngol Head Neck Surg 1992; 118: 940–3.
Wilson K, Lakheeram I, Morielli A, Brouillette R, Brown K. Can assessment for obstructive sleep apnea help predict postadenotonsillectomy respiratory complications? Anesthesiology 2002; 96: 313–22.
Parnis SJ, Barker DS, Van Der Walt JH. Clinical predictors of anaesthetic complications in children with respiratory tract infections. Paediatr Anaesth 2001; 11: 29–40.
Newland MC, Ellis SJ, Lydiatt CA, et al. Anestheticrelated cardiac arrest and its mortality. A report covering 72,959 anesthetics over 10 years from US teaching hospitals. Anesthesiology 2002; 97: 108–15.
Katz ES, Greene MG, Carson KA, et al. Night-to-night variability of polysomnography in children with suspected obstructive sleep apnea. J Pediatr 2002; 140: 589–94.
Jacob SV, Morielli A, Mograss MA, Ducharme FM, Schloss MD, Brouillette RT. Home testing for pediatric obstructive sleep apnea syndrome secondary to adenotonsillar hypertrophy. Pediatr Pulmonol 1995; 20: 241–52.
Brouillette RT, Morielli A, Leimanis A, Waters KA, Luciano R, Ducharme FM. Nocturnal pulse oximetry as an abbreviated testing modality for pediatric obstructive sleep apnea. Pediatrics 2000; 105: 405–12.
Waters KA, Forbes P, Morielli A, et al. Sleep-disordered breathing in children with myelomeningocele. J Pediatr 1998; 132: 672–81.
Morielli A, Ladan S, Ducharme FM, Brouillette RT. Can sleep and wakefulness be distinguished in children by cardiorespiratory and videotape recordings? Chest 1996; 109: 680–7.
Lafontaine VM, Ducharme FM, Brouillette RT. Pulse oximetry: accuracy of methods of interpreting graphic summaries. Pediatr Pulmonol 1996; 21: 121–31.
Tobias JD. Pain management for the critically ill child in the pediatric intensive care unit.Ln: Schechter NL, Berde CB, Yaster M (Eds.). Pain in Infants, Children, and Adolescents, 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003: 807–40.
Hosmer DW, Lemeshow S. Applied Logistic Regression, 2nd ed. New York: A Wiley-Interscience Publication; 2000.
Cohen MM, Cameron CB, Duncan PG. Pediatrie anesthesia morbidity and mortality in the perioperative period. Anesth Analg 1990; 70: 160–7.
Cohen MM, Cameron CB. Should you cancel the operation when a child has an upper respiratory tract infection? Anesth Analg 1991; 72: 282–8.
Helfaer MA, McColley SA, Pyzik PL, et al. Polysomnography after adenotonsillectomy in mild pediatric obstructive sleep apnea. Crit Care Med 1996; 24: 1323–7.
Suen JS, Arnold JE, Brooks LJ. Adenotonsillectomy for treatment of obstructive sleep apnea in children. Arch Otolaryngol Head Neck Surg 1995; 121: 525–30.
Marcus CL, Omlin KJ, Basinki DJ, et al. Normal polysomnographic values for children and adolescents. Am Rev Respir Dis 1992; 146: 1235–9.
Waters KA, McBrien F, Stewart P, Hinder M, Wharton S. Effects of OSA, inhalational anesthesia, and fentanyl on the airway and ventilation of children. J Appl Physiol 2002; 92: 1987–94.
Goh DY, Galster P, Marcus CL. Sleep architecture and respiratory disturbances in children with obstructive sleep apnea. Am J Respir Crit Care Med 2000; 162: 682–6.
Bell CM, Redelmeier DA. Mortality among patients admitted to hospitals on weekends as compared with weekdays. N Engl J Med 2001; 345: 663–8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Koomson, A., Morin, I., Brouillette, R. et al. Children with severe OSAS who have adenotonsillectomy in the morning are less likely to have postoperative desaturation than those operated in the afternoon. Can J Anesth 51, 62–67 (2004). https://doi.org/10.1007/BF03018549
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03018549