
Abstract
Purpose
We assessed the effect of cuff inflation of the laryngeal mask airway at removal on sore throat, pharyngeal morbidity and airway complications.
Methods
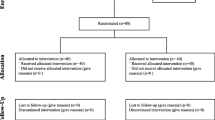
In a prospective randomized trial, we used a standardized technique of anesthesia and of laryngeal mask insertion in 126 consecutive day-case patients. Postoperatively, on eye opening, the masks were removed either inflated (Group A) or deflated (Group B) and examined for blood by a blinded observer. Episodes of coughing, gagging, laryngospasm, hiccups and retching, and symptoms of sore throat and hoarseness were recorded by the same observer.
Results
Demographics were similar. Bloodstaining occurred in 21% of patients in Group A (n = 63) vs 13% in Group B (n = 63;P = 0.23); the incidence of sore throat was identical (19%). Group A experienced more hoarseness (22% vs 9%;P = 0.05). Overall airway complications did not differ between groups (19% vs 11%;P = 0.21).
Conclusion
We conclude that removal of the laryngeal mask airway inflated does not reduce the incidence of sore throat, pharyngeal morbidity or airway complications.
Résumé
Objectif
Évaluer l’effet du gonflement du ballonnet du masque laryngé lors du retrait sur l’incidence de maux de gorge, sur la morbidité pharyngée et sur les complications touchant les voies respiratoires.
Méthode
Au cours d’un essai prospectif et randomisé, nous avons utilisé une technique normalisée d’anesthésie et d’insertion du masque laryngé chez 126 patients consécutifs en chirurgie d’un jour. Après l’opération, à l’ouverture des yeux, le masque était enlevé, soit en gardant le ballonnet gonflé (Groupe A), soit non gonflé (Groupe B) et examiné pour la présence possible de sang par un observateur impartial. Les épisodes de toux, de haut-le-cæur, laryngospasme et efforts pour vomir, et les symptômes de maux de gorge et de raucité de la voix ont été notés par le même observateur.
Résultats
Les données démographiques des patients étaient comparables. Des traces de sang ont été observées chez 21% des patients du Groupe A (n = 63) vs 13% du Groupe B (n = 63; P = 0,23); l’incidence de mal de gorge a été identique (19%). On a noté plus d’enrouement chez les patients du Groupe A(22% vs 9%; P = 0,05). L’ensemble des complications n’a pas présenté de différence intergroupe (19% vs 11%; P = 0,21).
Conclusion
Le retrait du masque laryngé dont le ballonnet est encore gonflé ne réduit pas l’incidence de mal de gorge, de morbidité pharyngée ou de complications des voies respiratoires.
Article PDF
Similar content being viewed by others


References
Morris GN, Marjot R. Laryngeal mask airway performance: effect of cuff deflation during anaesthesia. Br J Anaesth 1996; 76: 456–8.
Asai T, Brimacombe J. Cuff volume and size selection with the laryngeal mask. Anaesthesia 2000; 55: 1179–84.
Deakin CD, Diprose P, Majumdar R, Pulletz M. An investigation into the quantity of secretions removed by inflated and deflated laryngeal mask airways. Anaesthesia 2000; 55: 478–80.
Brimacombe J, Holyoake L, Keller C, et al. Emergence characteristics and postoperative laryngopharyngeal morbidity with the laryngeal mask airway: a comparison of high versus low initial cuff volume. Anaesthesia 2000; 55: 338–43.
Keller C, Sparr HJ, Brimacombe JR. Laryngeal mask lubrication. A comparative study of saline versus 2% lignocaine gel with cuff pressure control. Anaesthesia 1997; 52: 592–602.
Brimacombe JR, Brain AIJ, Berry AM. The Laryngeal Mask Airway Instruction Manual. 4th ed. London: Intavent Research Ltd., 1999.
Author information
Authors and Affiliations
Corresponding author
Additional information
Note: No grants or financial support were received by the authors in the conduct of this study.
Rights and permissions
About this article
Cite this article
O’Brien, B., Harmon, D., Duggan, M. et al. Laryngeal mask cuff inflation at removal does not affect early postoperative laryngopharyngeal morbidity. Can J Anesth 49, 871–873 (2002). https://doi.org/10.1007/BF03017423
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03017423